This reference is authored by Dr. Meng, Howard - May 2024
Lumbar Erector Spinae Plane Block
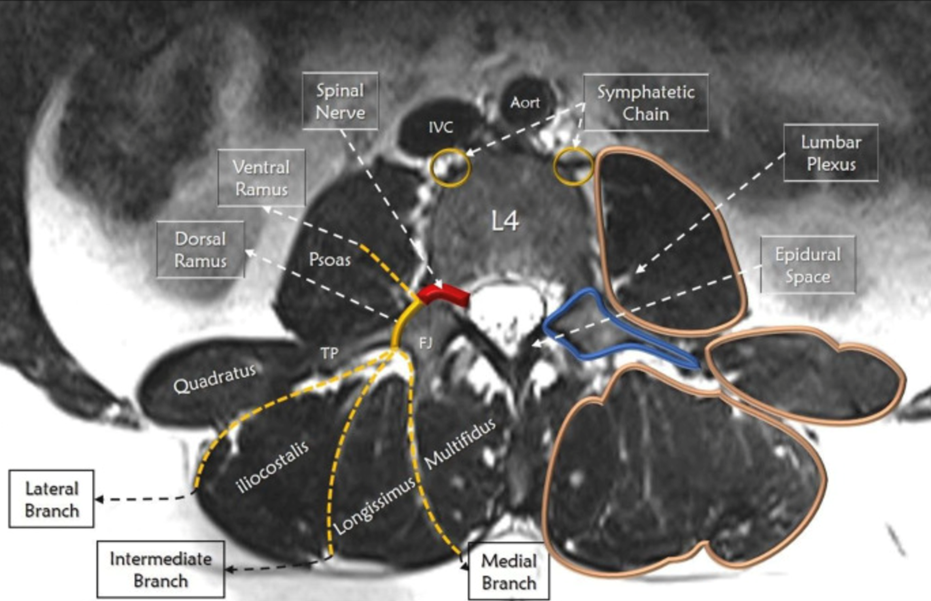
Ultrasound guided lumbar erector spinae plane block has been identified to be an effective intervention for analgesia in lumbar spine surgery. The interfascial plane block aims to block afferent conduction of pain signals at the dorsal rami of the spinal nerves. The intended goal is to provide sensory blockade (dorsal ramus) without motor blockade (ventral ramus).
Goal: Provide optimal anagelsia post-lumbar spine surgery and facilitate early discharge from hospital.
Challenges
Some patients have inappropriate spread of local anesthetic to the ventral branch of the spinal nerve resulting in motor deficit for several hours after surgery
Patients for repeat lumbar spine surgery have hardware and scar tissue that results in suboptimal visualization of target under ultrasound and unreliable spread of local anesthetic respectively
Image Acquisition
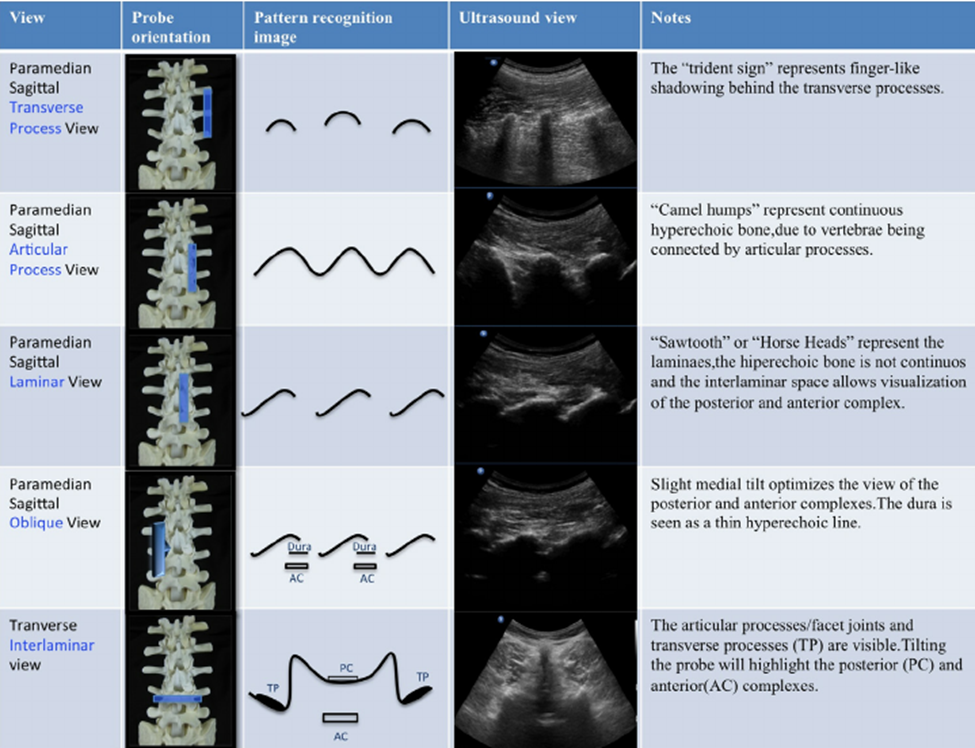
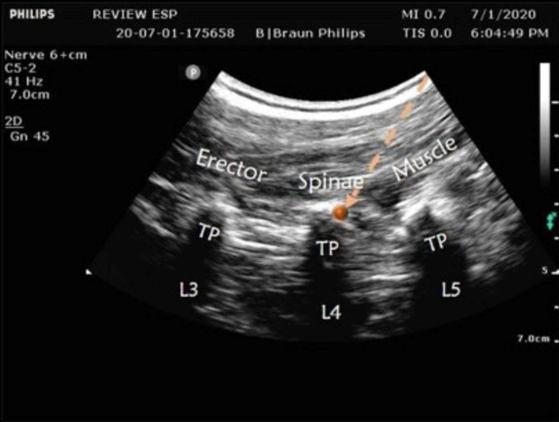
Scan with curvilinear probe in longitudinal orientation starting from sacrum
Translate probe cephalad to the level of surgery
Identify one level either cephalad or caudad to the level of surgery i.e. L3 for L4/5 fusion – target for needle-bone contact
Translate probe medially and laterally to visualize for the transverse process (TP)
Procedure
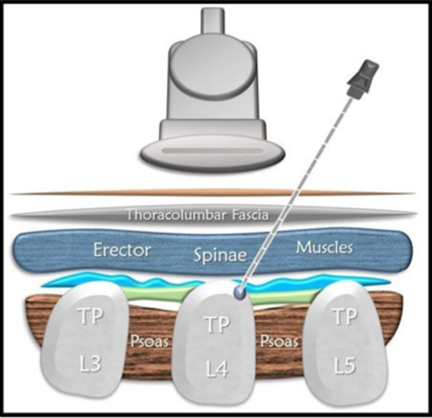
22g 80mm echogenic needle
In-plane approach with sagittal/longitudinal view
Use no more than 15cc of injectate on each side (10cc adequate)
Injectate should not be more concentrated than 0.25% bupivacaine or 0.25% ropivacaine
Use of epinephrine (1:400 000) is at the practitioner’s discretion
Technical Considerations
Ensure needle contact with TP one level away from the surgical level
Contact the TP at the mid-point rather than at the edge which can result in injection deep to the desired plane
Ensure the probe is oriented in a sagittal/longitudinal plane that allows for visualization of several levels of TPs (patient may be lying with slight lateral flexion)
Spread of the local anesthetic should easily traverse 1-2 vertebral levels. Adjust needle and probe as necessary if spread is not achieved. Call for help if needed.
TLIP (Thoracolumbar Interfascial Plane Block)
In patients with lumbar spine hardware or difficult to visualize anatomy for ESP block, consider performing the TLIP block
TLIP provides analgesia via similar mechanism as the lumbar ESP block
The block can be done at the level of the surgery
Use no more than 15cc of injectate
See below for Youtube link for performance of TLIP block by Dr. Ki Jinn Chin from Toronto Western Hospital

No Comments