Generally with Placenta Accreta Spectrum (PAS), the obstetrical plan is Cesarean section with / without hysterectomy. If possible, these cases are done electively in main OR on M2
Key Players: Main OR Anesthesia, OB anesthesia, Obstetrics, Gynecology, Urogynecology, MFM, Urology, Hematologist, Blood Bank, Interventional Radiology, Neonatologist
Plan A – Scheduled Ceasarean +/- hysterectomy in Main OR
2 staff obstetricians
NICU will transport necessary equipment/medications and have appropriate personnel in main OR.
If Possible CSE initially for delivery of baby. It will be up to the Anesthesiologist to determine if the hysterectomy should continue under regional anesthesia or if conversion to GA will be necessary.
Plan B – Urgent indication for OR
If case becomes urgent (likely scenario being patient begins contracting, bleeding persistently or suddenly and/or needing more than 1 transfusion/day), case will be booked as an A case and patient will be transferred to main OR if available.
Obstetrics on call with Gyne backup to perform Ceasarean. Urology to be called if needed.
Main OR Anesthesiologist will lead this case with OB Anesthesiology consultation/backup.
Cell Saver (perfusionist or AA) depending on call schedule.
Method of anesthesia at the discretion of the on-call Anesthesiologists.
NICU to bring warmer and appropriate personnel/equipment.
Plan C – Emergency indication for OR
If sudden hemorrhage occurs that yields the patient too unstable for transport, the case will be done on M5 L&D, and appropriate services and equipment (surgical equipment) will be transferred up to L&D OR.
OB Anesthesiology will lead this case. Main OR Anesthesiology will be backup.
Method of anesthesia at the discretion of the on-call Anesthesiologists.
Perfusionist and/or AA will also be called in for cell saver.
RRT (rapid response team) may also be a resource in extreme circumstances.
OR / Personnel Setup:
Call blood bank to ensure adequate cross-matched units available (in main OR fridge or in OR). Prepare for massive transfusion protocol/code transfusion OB.
Call in personnel for cell salvage. Note that AA’s and perfusionists rotate on a q-monthly basis for cell saver call. If perfusion team is responsible for cell salvage, AA’s will still need to be called in for assistance.
Cell salvage should only be initiated AFTER baby is delivered, after amniotic fluid is suctioned with a separate system, and with the use of appropriate filtration system.
Request that scrubbed nursing team rinse bloody sponges in saline and pass along for cell salvage.
Recommend Level 1 Rapid Infuser in room and primed.
Advise CRCU of potential admission.
Induction of Anesthesia
Ensure patient is in left lateral tilt position to prevent aorto-caval compression until baby is delivered. This is usually performed with a flannel rolled and place under right side of patient or slight tilting of bed.
Mode of anesthesia to be judged on a case by case basis. If high likelihood of massive hemorrhage, coagulopathy, fluid resuscitation leading to airway edema, suggest general anesthesia from the start. If patient is stable and there are no contraindications than a CSE +/-conversion to general anesthesia after delivery of baby.
Invasive lines: recommend awake placement in order to minimize exposure of volatile/meds to fetus. Arterial line, IV access (multiple large bore IV, RIC’s, cordis) for massive hemorrhage, keeping in mind that induction to delivery time should be short as possible. May prefer to be done awake.
Before performing RSI for GA:
NICU must be in the room and aware of time of induction.
Surgeons must be prepped and draped.
Minimal time between ETT placement and incision with goal to minimize exposure of baby to anesthetic.
Have short laryngoscope handle and normal available, size 7.0 and 6.0 ETT with stylets and additional difficult airway equipment as needed.
TXA – 1 g prior at first incision. Repeat 1g 30min after initial dose if bleeding concerning. Some Obstetricians may prefer delay of initial dose until after delivery of baby. Recommend discussion before induction of case.
Anesthesia Maintenance
Before baby is delivered, maintain anesthesia with 50% 02, 50% nitrous oxide and ~Sevo 1.0.
After baby is delivered, maintain anesthesia with 30% 02, 70% nitrous oxide and lower MAC volatile 3. (~Sevo 0.5). This is to prevent uterine atony and further hemorrhage. Supplement with IV anesthetics as needed.
Once uterus is removed, risk of atony and related hemorrhage is also gone and one can resume anesthesia as tolerated.
Uterotonic Agents
Immediately after delivery of baby, administer small, diluted bolus of oxytocin (~1-2U via IV push) + an oxytocin infusion (usually 20-40U injected into 1L bag of LR running at a moderate rate with goal to be infused over ~1hr).
If performing C-hysterectomy, stop oxytocin once the uterus is out and hysterectomy is completed.
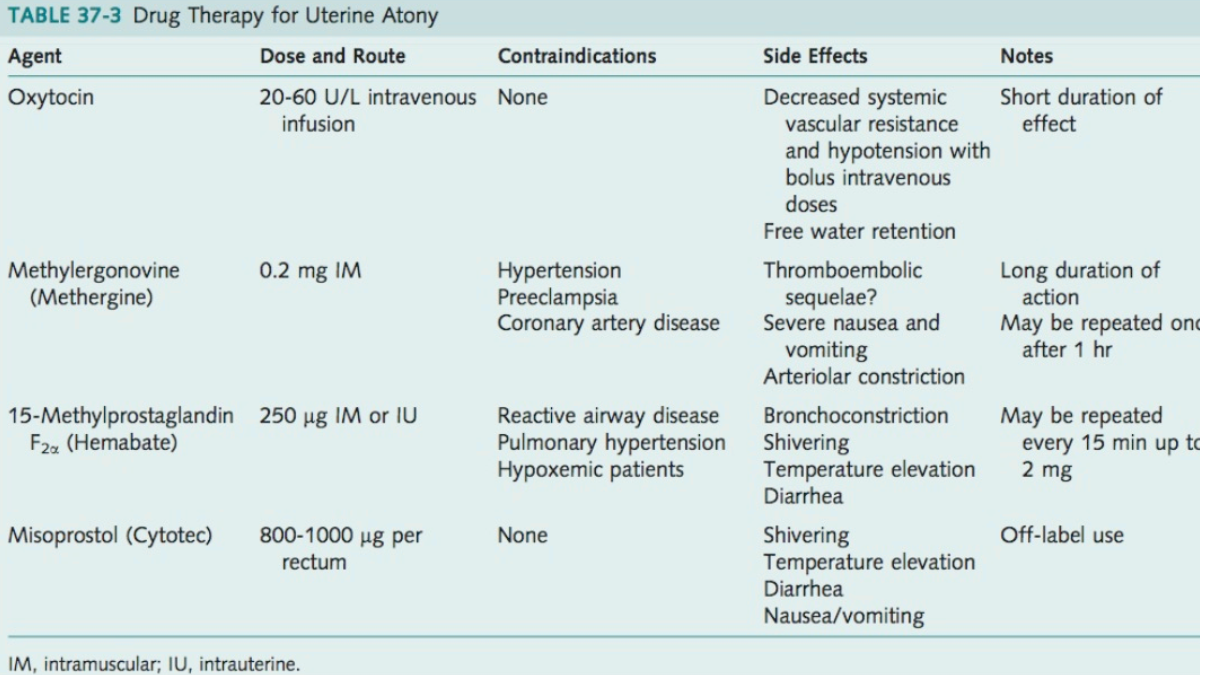
A postpartum hemorrhage kit (containing oxytocin, carboprost (Hemabate), methylergonovine (Ergot), misoprostol) is available in OR fridge on M2, and additional oxytocin is available at M2 OR core.
Although unlikely to be required in the setting of a Cesarean hysterectomy, appropriate dosing and administration of these medications are as follows:
Blood Products
Blood bank will ideally be involved with these patients early on and deliver appropriately cross-matched products.
It is common for these women to go into rapid DIC, so perform regular blood work (q1hr at least) assessing CBC, coagulation, and fibrinogen to guide transfusion therapy.
As with trauma, maintain a fibrinogen >2 mg/dL.
Fibrinogen concentrate or Cryopreciptiate will arrive earlier in an Obstetrics Code Transfusion in order to achieve this goal.

No Comments