Cardiac output increases by 50% by 2nd trimester w/ increased HR & SV
Blood volume increases by 45% --> dilutional anemia
Hypercoagulable state --> increases risks of periop thromboembolic events
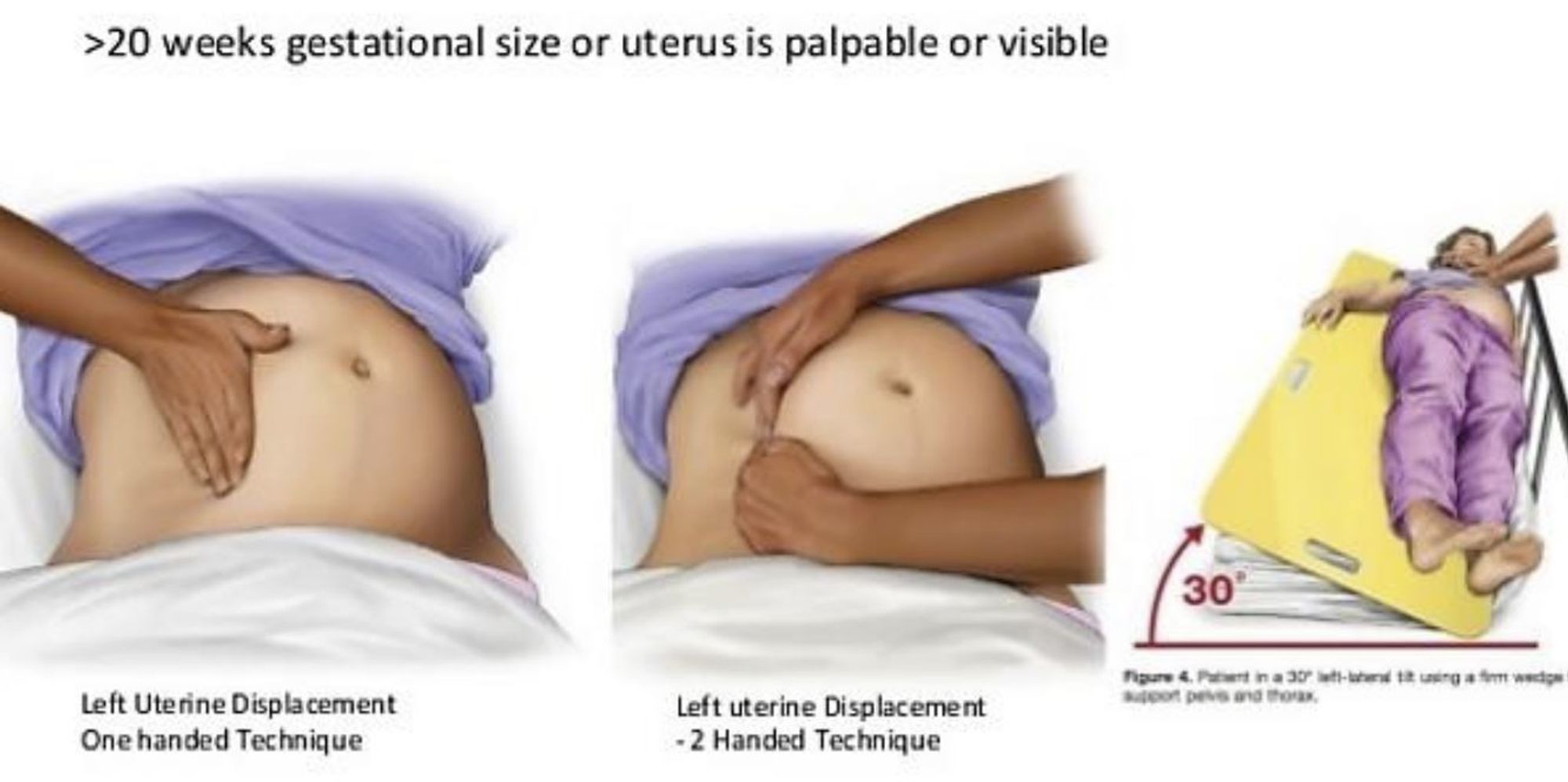
Aorto-caval compression w/ supine position --> oblique position for left uterine displacement --> prevents decrease in uterine blood flow and maternal hypotension
O2 consumption increases by 60%
Minute ventilation increases by 45% by increasing TV
FRC decreases by 20% (30% in supine) --> decreased safe duration of apnea
Delayed gastric emptying & increased intraabdominal pressure --> GERD --> aspiration prophylaxis e.g. 30ml NaCitrate, 10mg metoclopramide IV, 50mg ranitidine IV; RSI w/ cricoid pressure in case of GA
Reduced MAC by 30%
Reduced LA requirement by 25%
Renal blood flow increased by 75% --> GFR increased by 50%
Airway w/ internal and external edema --> potential difficult airway
Pulmonary edema - uncommon; reduced colloid oncotic pressure, endothelial dysfunction and diastolic dysfunction predisposed to development of pulmonary edema
CNS involvements e.g. cerebral edema, ICH, increased ICP, HA, visual disturbance, altered mentation, seizure
Hypertension, labile BP --> Art line prior to GA induction; NTG, phenylephrine readily available during induction; hypertensive crisis, LV dysfunction / cardiomyopathy / CHF
Reduced intravascular volume --> cautious with neuraxial blockade; volume expansion prior to spinal/epidural; phenylephrine readily available
Coagulopathy --> early insertion of epidural catheter before any coagulopathy, epidural is also partially therapeutic
50-70: risk vs benefit judgement (consider trend, other competing factors e.g. airway, cardiac / neuro status)
>70: likely safe
Renal impairment due to glomerular endotheliosis
Uteroplacental unit; increased chance of abruptio placenta
Risks to baby: IUGR, increased risk of fetal asphyxia, IUD, prematurity
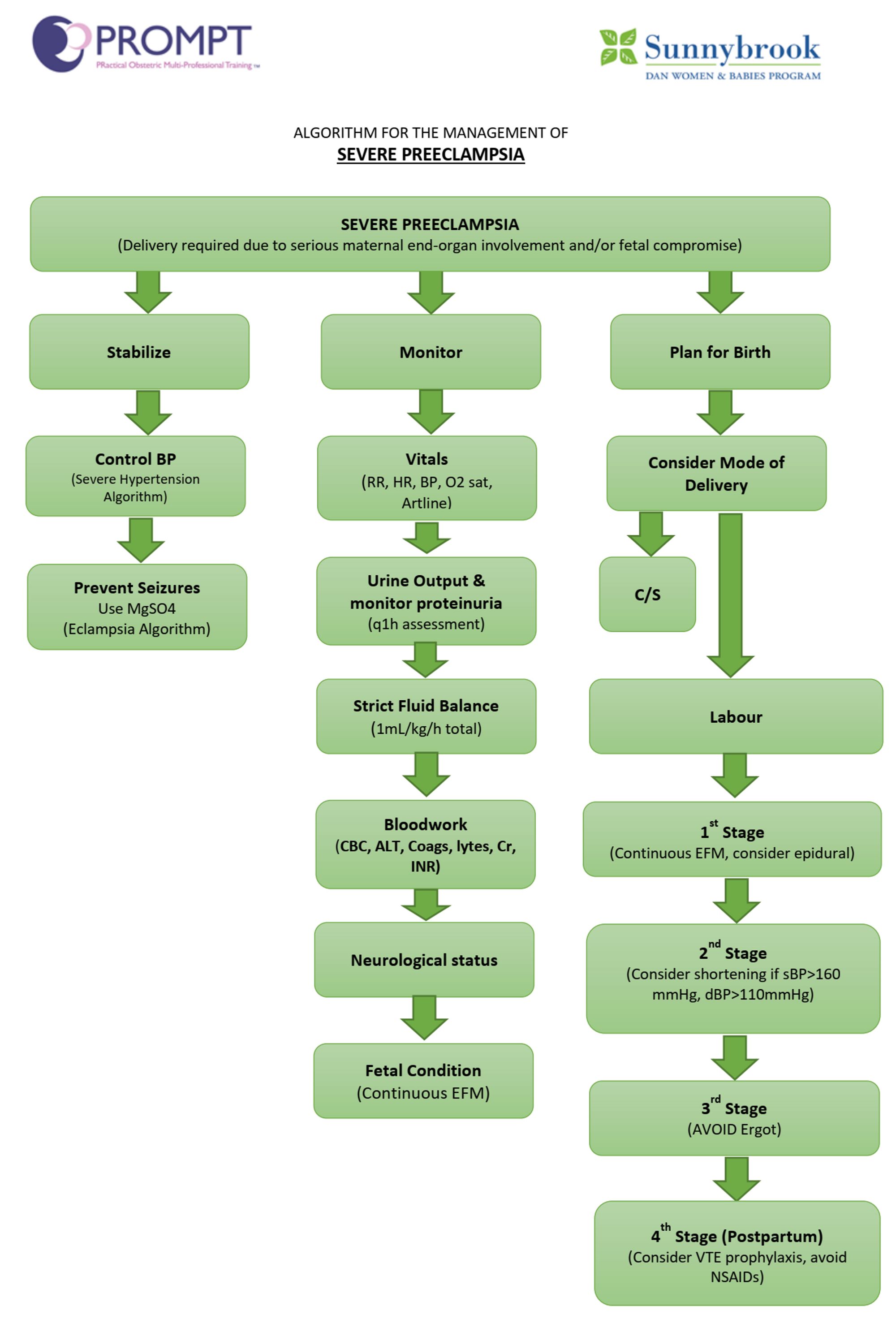
Goals:
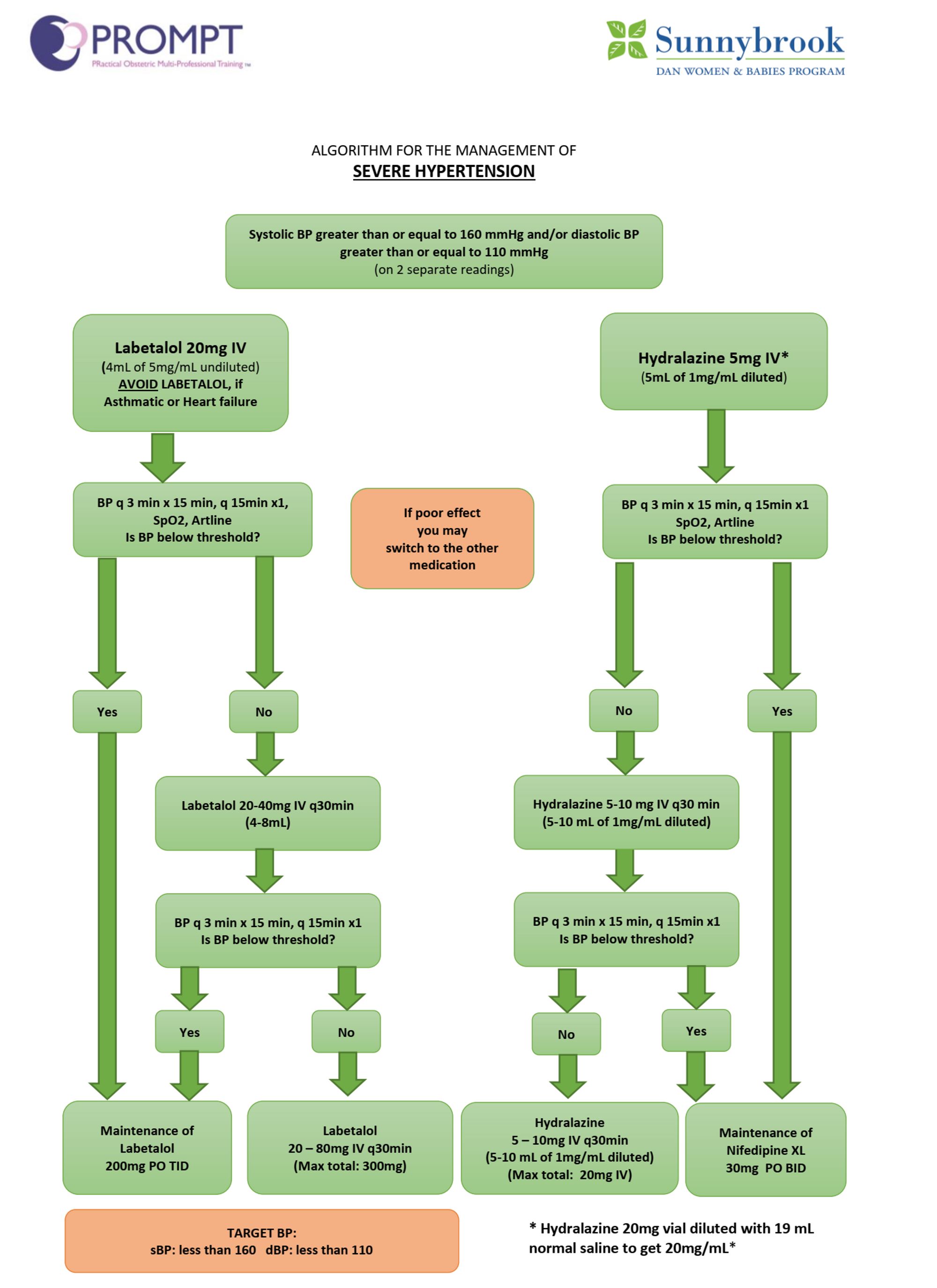
BP control (sBP <160 mmHg, dBP <110 mmHg)
Optimize volume status
Maintain adequate uteroplacental perfusion
Minimize end-organ issues e.g. seizures, ICH, cardiac ischemia
Optimize labour analgesia to minimize exacerbation of BP due to pain
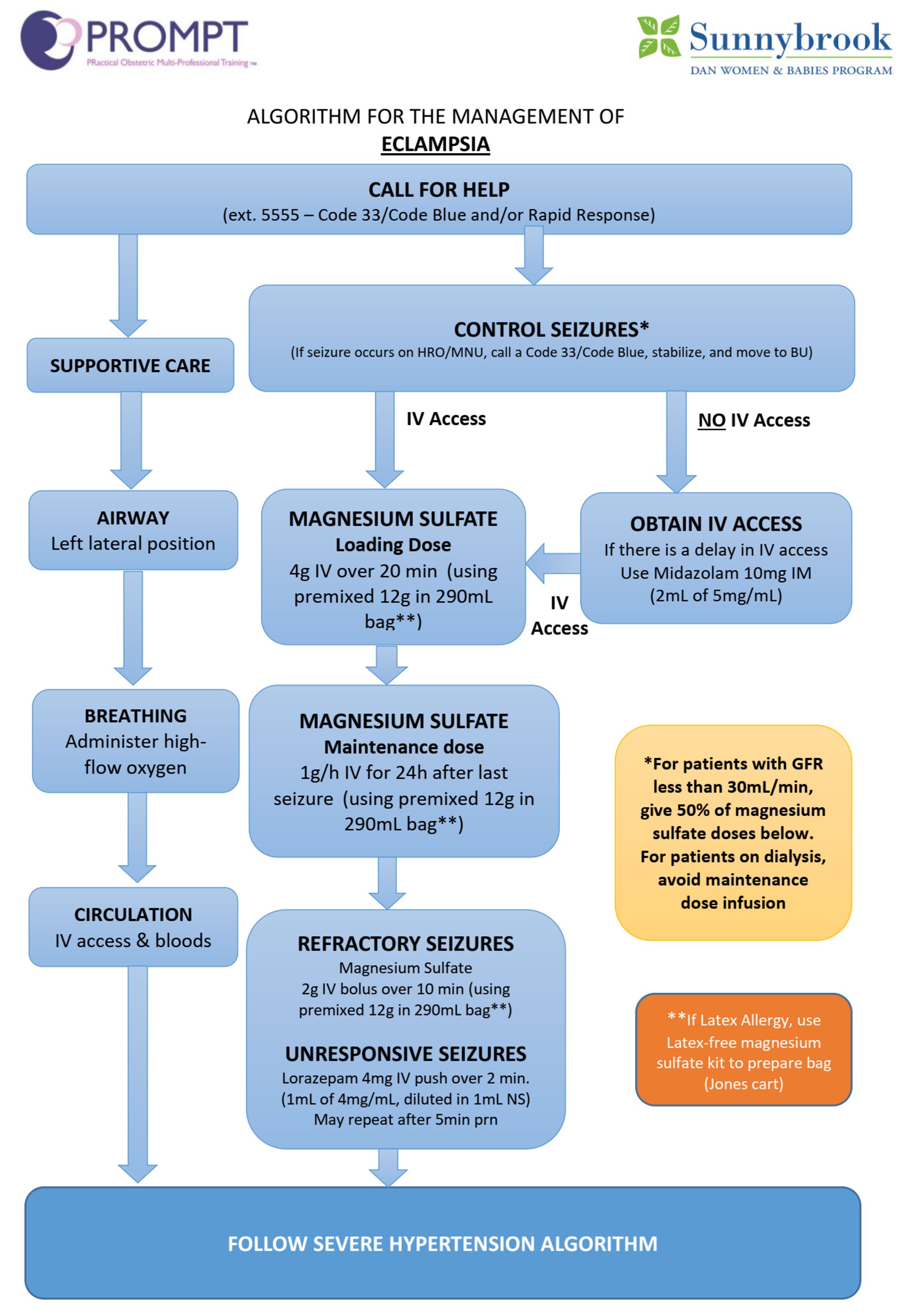
Pharmacological intervention:
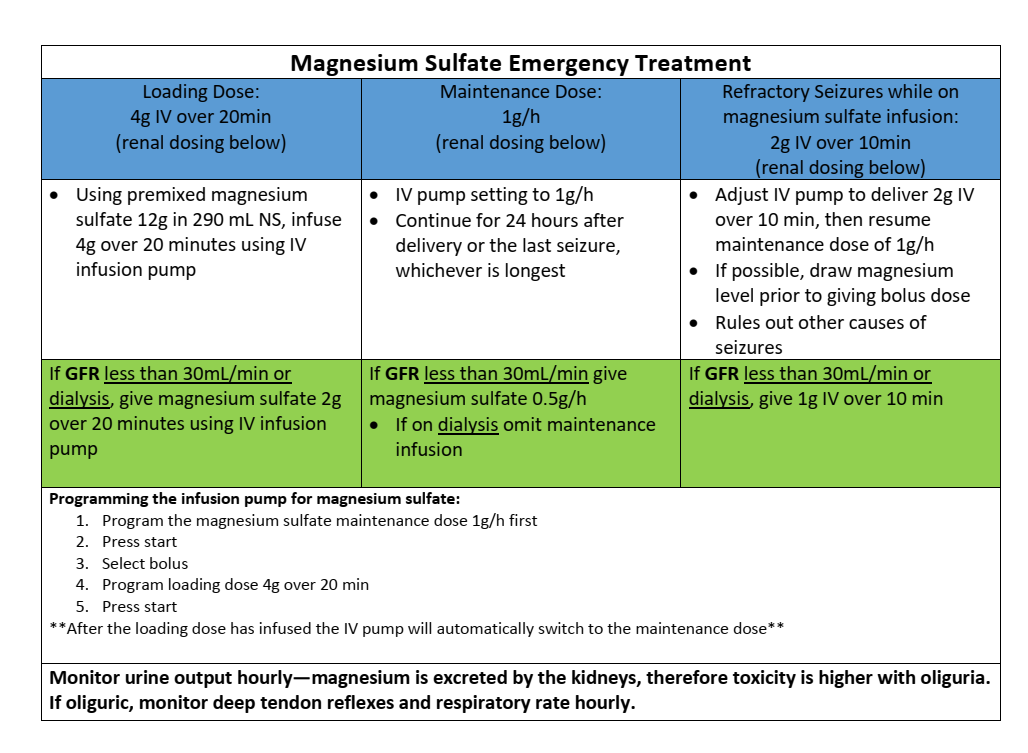
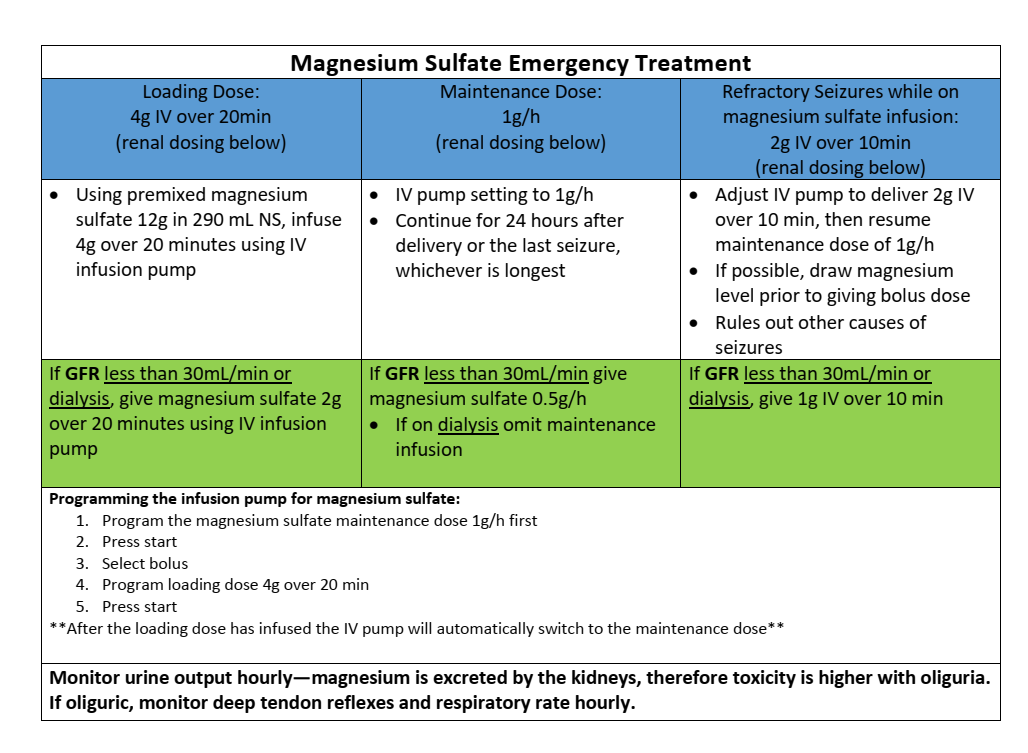
MgSO4 4g IV over 10-15min, then 1-3g per hour for maintenance; constant monitoring of cardiopulmonary status, knees DTR, urine output; Ca gluconate 1g IV over 3-5min in case of overdose
MgSO4 also for neuroprotection in premature babies
Hyralazine 5-10mg IV bolus, then 5mg per hour
Labetolol 20mg IV repeated q15min prn, 20mg/hr maintenance
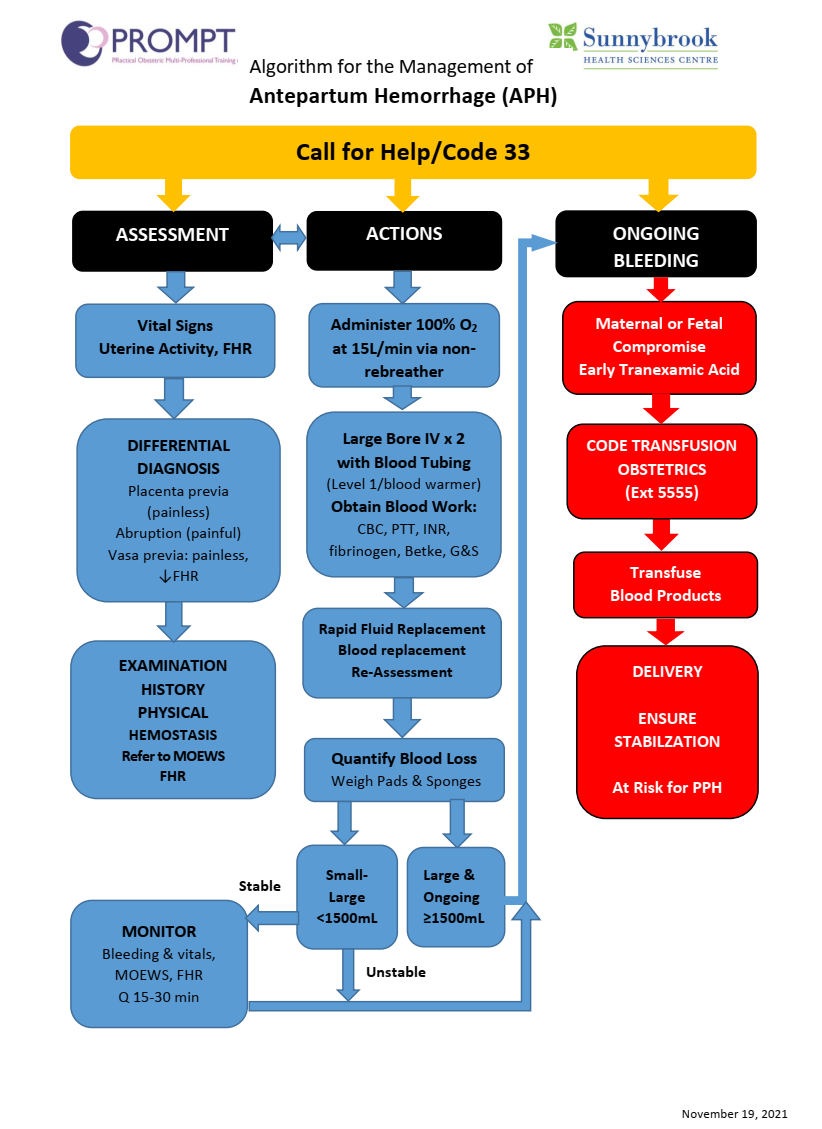
Antepartum Hemorrhage
Placenta Previa
Access severity i.e. Total, partial or marginal; Anterior vs posterior
Dx – painless vaginal bleeding, confirm with u/s, no vaginal exam
Anesthetic management
Elective vs urgent / embergent C-sectioin
AMPLE hx / px / labs
Cross & Type
Large bore IV access x 2
Risk of bleeding due to cutting into placenta, poor contraction of the lower uterine segment & increased risk of accreta
Regional – if hemodynamically stable & not actively bleeding; fetus stable to allow time for neuraxial technique
Vasa Previa
Rare cause of APH
Abnormal insertion of umbilical cord into the chorioamnion such that vessels run some distance within the amniotic membranes – primary risk is fetal hemorrhage / exanguination
Presents as vaginal bleeding with FHR changes (tachy followed by brady)
Fetal distress is disproportionate to the amount of bleeding
Emergent C-section
Elective C-section if diagnosis made antenatally
Placental Abruption
Access severity, amount of blood loss, fetal / maternal status
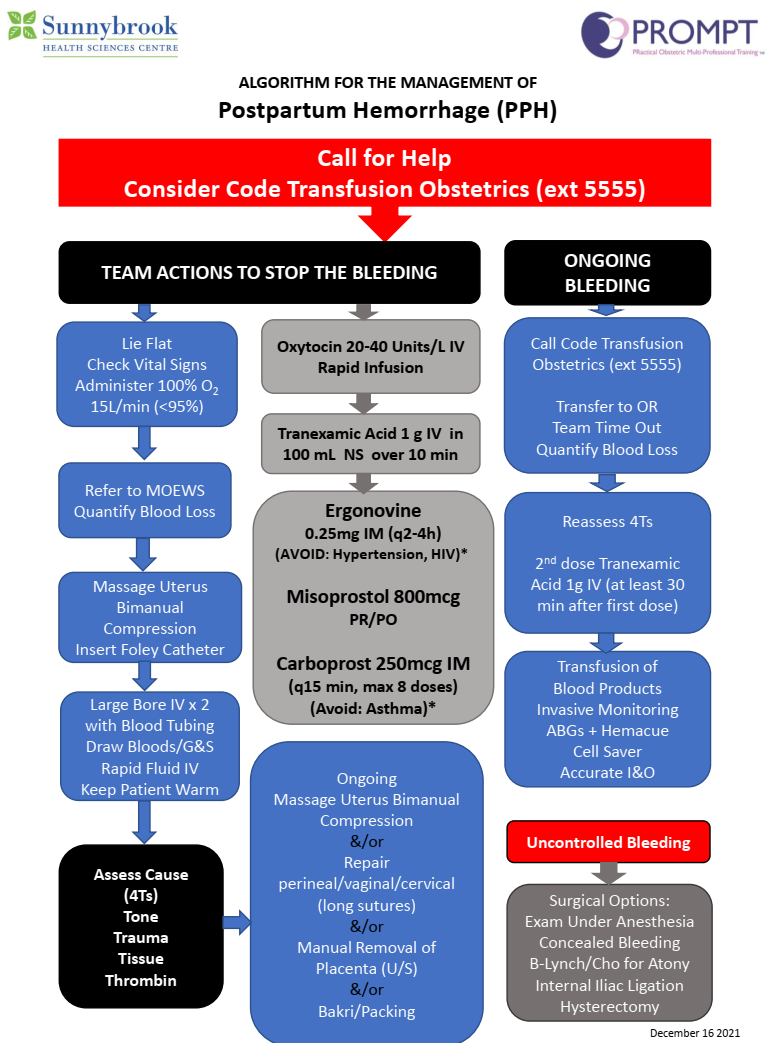
Oxytocin 5U slow bolus, then maximum 40U/L IV infusion; watch out for anaphylactoid reactions (hypotension, pruitus, urticaria, facial flusing, N/V)
Ergot 0.125-0.25 mg IV/IM w/ maximum dose 1.25mg; watch out for hypertension, increased CVP, coronary spasm, MI, arrythymia, bronchospasm, N/V; patients w/ CAD are contraindicated
Hemabate 0.25mg IM/IMM q15min; maximum 8 doses; watch out for N/V, bronchospasm, diarrhea, HTN, HA, flushing, diaphoresis, restlessness, pulmonary vasoconstriction
Consider surgical control: uterine massage, B lynch suture, packing, uterine artery ligation, IR embolization, hysterectomy
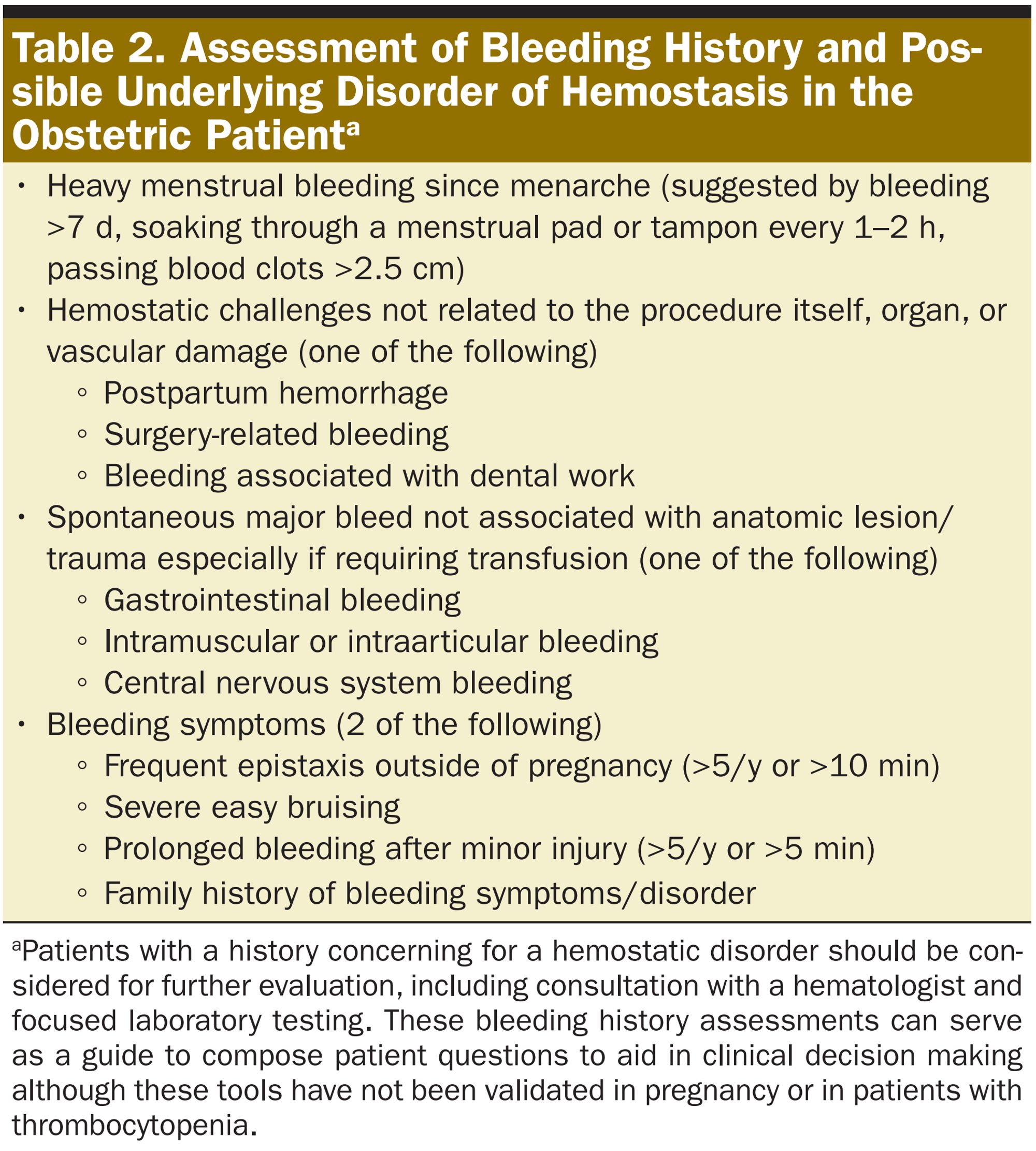
Thrombocytopenia
2024 CAS Guideline
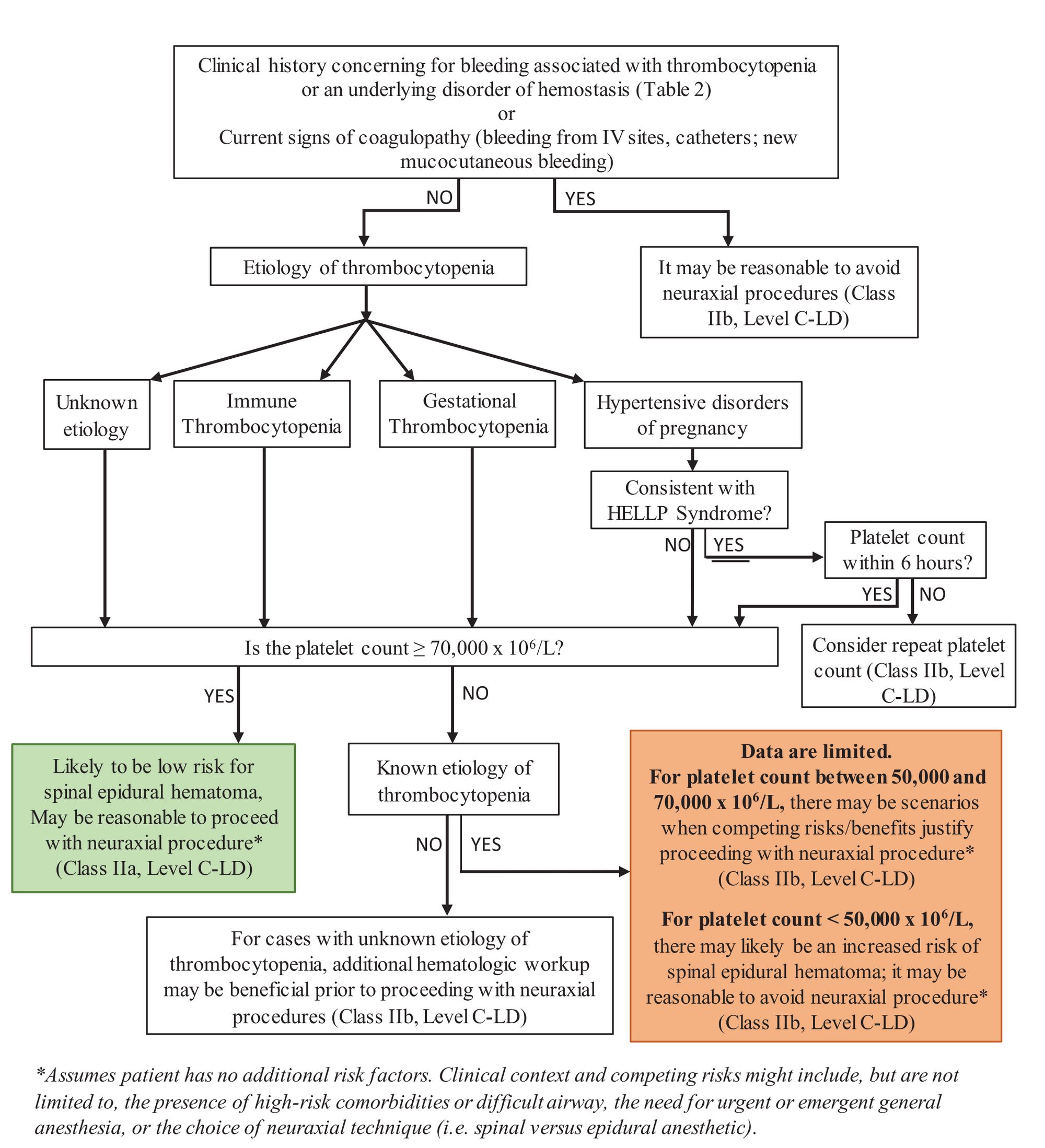
In a pregnant patient with a clinical history, physical exam, or laboratory results indicating thrombocytopenia (platelet count < 100x109/L), the anesthesiologist should determine if the patient has a qualitative defect (i.e., a problem with platelet structure or function) or an active coagulopathy that would contraindicate a neuraxial technique. [in the guideline, there is no elaboration on what tests / history / physical one would employ to determine such qualitative defect]
In a pregnant patient with suspected qualitative defects or active coagulopathy, it may be reasonable to avoid a neuraxial technique or to seek expert hematologic consultation before proceeding with the neuraxial technique.
Pregnant patient with isolated thrombocytopenia with no other associated signs of a qualitative defect or an active coagulopathy
platelet counts greater or equal to 70x109/L, there may be a low risk fo spinal epidural hematoma and it is reasonable to proceed with a neuraxial technique
platelet counts between 50 and 70x109/L, the anesthesiologist should consider the risks and benefits of proceeding or avoiding a neuraxial technique and share the decision-making with the patient. Factors to consider: etiology of thrombocytopenia, trend of platelet count over time, patient comorbidities, Ob risk factors, airway and back examination, the risk of GA and patient preference.
platelet counts of < 50x109/L, there may be an increased risk of subdural or epidural hematoma and it is reasonable to avoid a neuraxial technique.
SOAP Interdisciplinary Consensus Statement on Neuraxial Procedures in Obstetric Patients With Thrombocytopenia; Anesthesia Analgesia 2021
Etiologies:
Gestational thromobocytopenia; incidence during pregnancy 5-11%, onset late 2nd or 3rd tremester, platelet count >75000, generally asymptomatic
Preeclampsia; incidence 5-8%, onset late 2nd or 3rd trimester
HELLP syndrome; incidence <1%, 70% onset later 2nd or 3rd trimester, 30% onset postpartum, 15%–20% of cases no hypertension or proteinuria, platelet count nadir occurs 24–48 h after delivery
ITP; incidence <1%, onset at any trimester, thrombocytopenia outside of pregnancy possible, platelet count <100,000 ± large platelets on blood smear, rarely may have signs of bleeding, bruising, and petechiae
Other rare causes: acute fatty liver of pregnancy, TTP, sepsis-induced thrombocytopenia; not covered by the consensus statement
Incidence of spinal epidural hematoma in the general obstetric population 1:200,000 to 1:250,000; incidence in obstetric patients with thrombocytopenia (<100,000) is unknown; retrospective studies suggest incidence of 0.19% (plt count 70,000 - 100,000), 2.6% (plt 50,000 - 69,000) & 9% (plt < 50,000)
Other than platelet count on CBC, no other lab test (including PFA-100, TEG or ROTEM) can reliably assess platelet function or bleeding risk
First assess for any clinical history of abnormal bleeding, any signs of DIC (bleeding from IV sites, catheters, wounds, or new mucocutaneous bleeding)
Decision Algorithm
Platelets transfusion:
Not recommended for the sole purpose of neuraxial technique
ACOG recommends platelet transfusion in preeclampsia for active bleeding or to improve the platelet count to 50,000 before cesarean delivery
IVIG & steroid are treatment of choice for ITP
Platelet transfusions are recommended to temporize only in cases of life-threatening hemorrhage or to prepare for urgent surgery because the response to platelet transfusion is short-lived
Insufficient evidence to make recommendation regarding neuraxial procedures in obstetric patients with thrombocytopenia who are also taking aspirin concurrently
Ultimately, the decision of whether or not to proceed with a neuraxial procedure in an obstetric patient with thrombocytopenia occurs in a clinical context with relevant factors that include maternal comorbidities and airway examination, obstetric risk factors, available airway equipment, type of neuraxial procedure, and patient preference
Placenta Accreta
Urgency depending on presentation; can range from elective to emergency
Risk factors:
Multiple previous C-sections
Placenta previa
Multiparity
Advanced maternal age > 35
History of uterine surgery e.g. myomectomy
Significantly increases likelihood of PPH especially with percreta or increta with neighboring organ e.g. urinary bladder invasion
Elective C-section
Preop consultation for adequate optimization e.g. hemoglobin and discussion of anesthetic plans; consider blood conservation clinic
Liaise with OB team to clarify severity of accreta, plan for uterus perservation or Cesarean hysterectomy
Consult other specialty e.g. urology or general surgery in cases of percreta
Consult NICU
ICU or step down monitored bed for post op care
Case generally done in main OR for easier access for additional equipments, personnels and surgeons
Urgent
Likely scenarios e.g. patient goes into labor, bleeding persistently or suddenly and/or needing more than 1 transfusion/day
Obstetrics on call to notify Gyne as backup to perform Ceasarean. Urology to be called if needed
NICU to bring warmer and appropriate personnel/equipment
Call for help e.g. AA, another anesthesiologist
Liasie with blood bank for potential massive transfusion
Emergent
Similar to Urgent
Sudden hemorrhage occurs that renders the patient too unstable to transfer to main OR from L&D, the case should then be done on L&D, and appropriate services and surgical equipment will be transferred up to L&D OR
Activate code Ob massive transfusion
Notify ICU
OR/Personnel Setup:
Arrange cell saver - cell salvage should only be initiated AFTER baby is delivered, after amniotic fluid is suctioned with a separate system, and with the use of appropriate filtration system
Level 1 rapid Infuser primed
Induction of Anesthesia:
Ensure patient is in left lateral tilt to prevent aorto-caval compression until baby is delivered
Mode of anesthesia to be judged on a case by case basis depending on the urgency and other factors:
If high likelihood of massive hemorrhage, coagulopathy, fluid resuscitation leading to airway edema, suggest general anesthesia from the start
If patient is stable and there is no contraindications, then a CSE +/-conversion to general anesthesia after delivery of baby
If GA from the outset, concurrent surgical prep during pre-oxygenation to minimize exposure of volatile/meds to fetus. Minimal time between intubation and incision with goal to minimize exposure of baby to anesthetic.
Arterial line, large bore IV or central venous line
NICU must be in the room
Short laryngoscope handle available, size 7.0 and 6.0 ETT with stylets with additional difficult airway equipment as needed
TXA 1g prior prior to incision. Repeat 1g 30min after initial dose if bleeding is concerning
Maintainence of Anesthesia:
Before baby is delivered - maintain anesthesia with 50% 02, 50% nitrous oxide and ~Sevo 1.0
After baby is delivered - maintain with 30% 02, 70% nitrous oxide and lower MAC volatile ~Sevo 0.5 to minimize uterine atony and further hemorrhage
Supplement with IV anesthetics as needed
Once uterus is removed, risk of atony and related hemorrhage is also gone and one can resume 'regular' anesthesia as tolerated
Urotonic agents after delivery of baby
It is common for these patients to go into rapid DIC, so perform regular blood work (q1hr at least) assessing CBC, coagulation, and fibrinogen to guide transfusion therapy
Goal to avoid delay in diagnosis and to intitiate early treatment
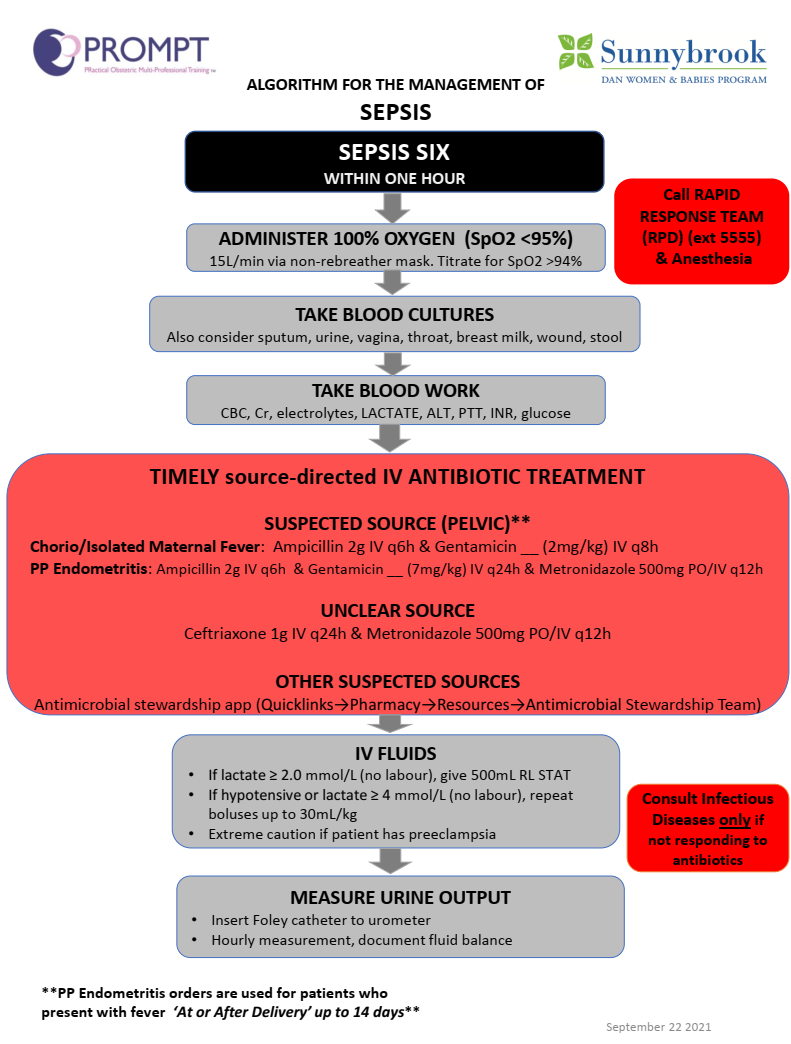
Organ dysfunction resulting from infection during pregnancy, childbirth, postabortion, or postpartum period (up to 42 days postpartum)
Second leading cause of maternal death in the United States; ~ 12% of all pregnancy related deaths; 23% of in-hospital maternal deaths, 45% of which occurred during postpartum readmission (mean interval of 13 days after initial discharge)
Patients and families should receive discharge information on the symptoms and signs of infection and sepsis (e.g. pyrexia, nonhealing incision, increasing pain, erythema or drainage from incision, foul-smelling discharge)
Antepartum sepsis most commonly originates from nonpelvic source e.g. pneumonia, whereas intrapartum and postpartum cases are more commonly related to pelvic source e.g. GU; 30% of cases, source is not identified
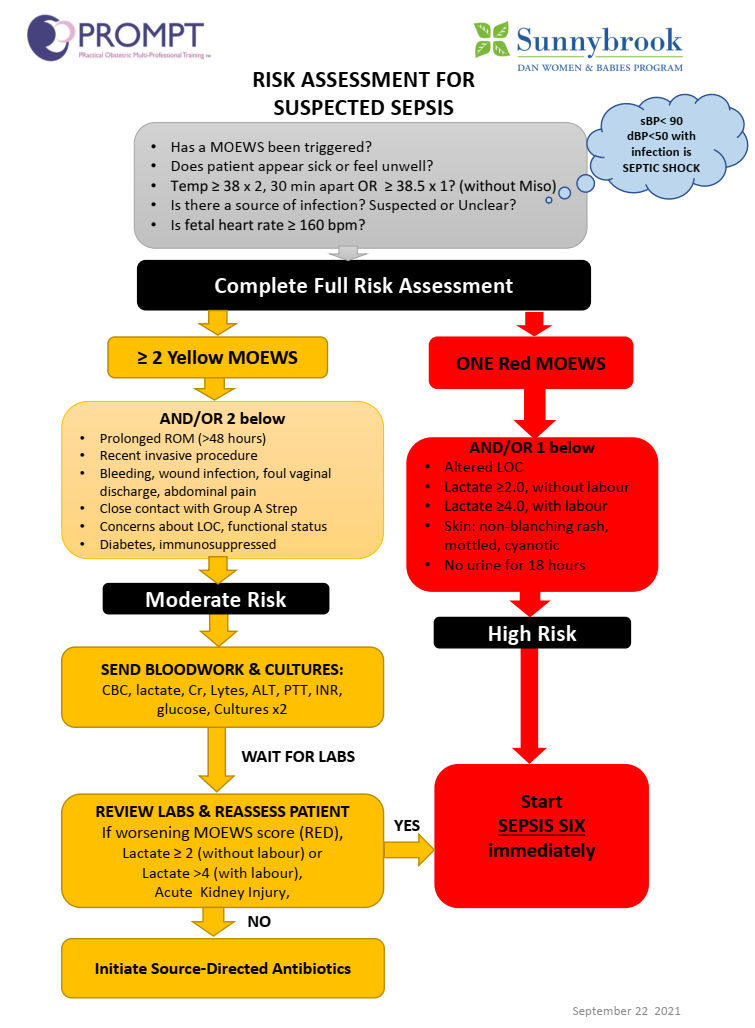
Maintain high level of suspicion: Does the parturient look sick or feel unwell? Is there a source of infection e.g. PPROM, pyelonephritis, pneumonia? Is the fetal heart rate ≥ 160 bpm
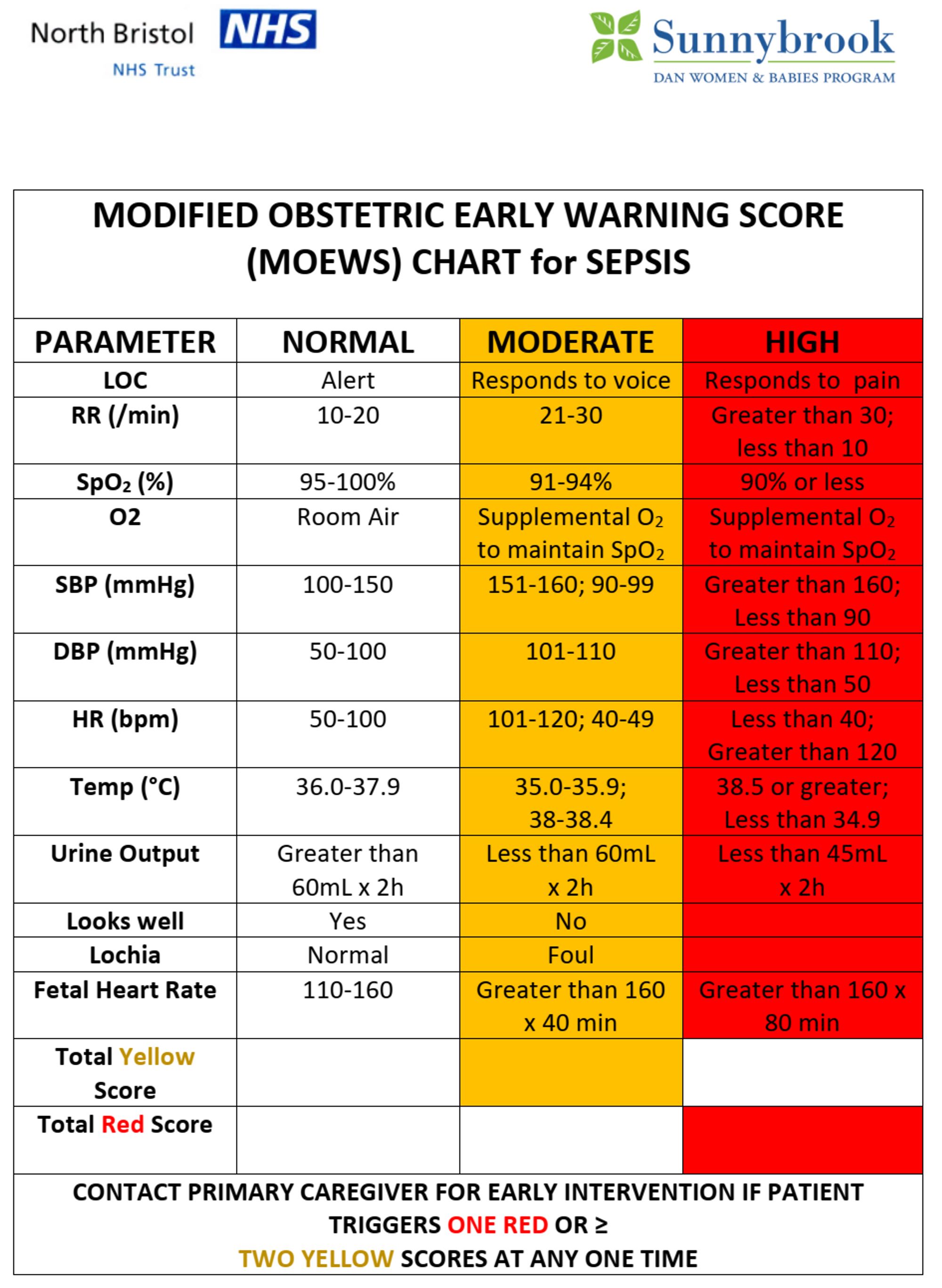
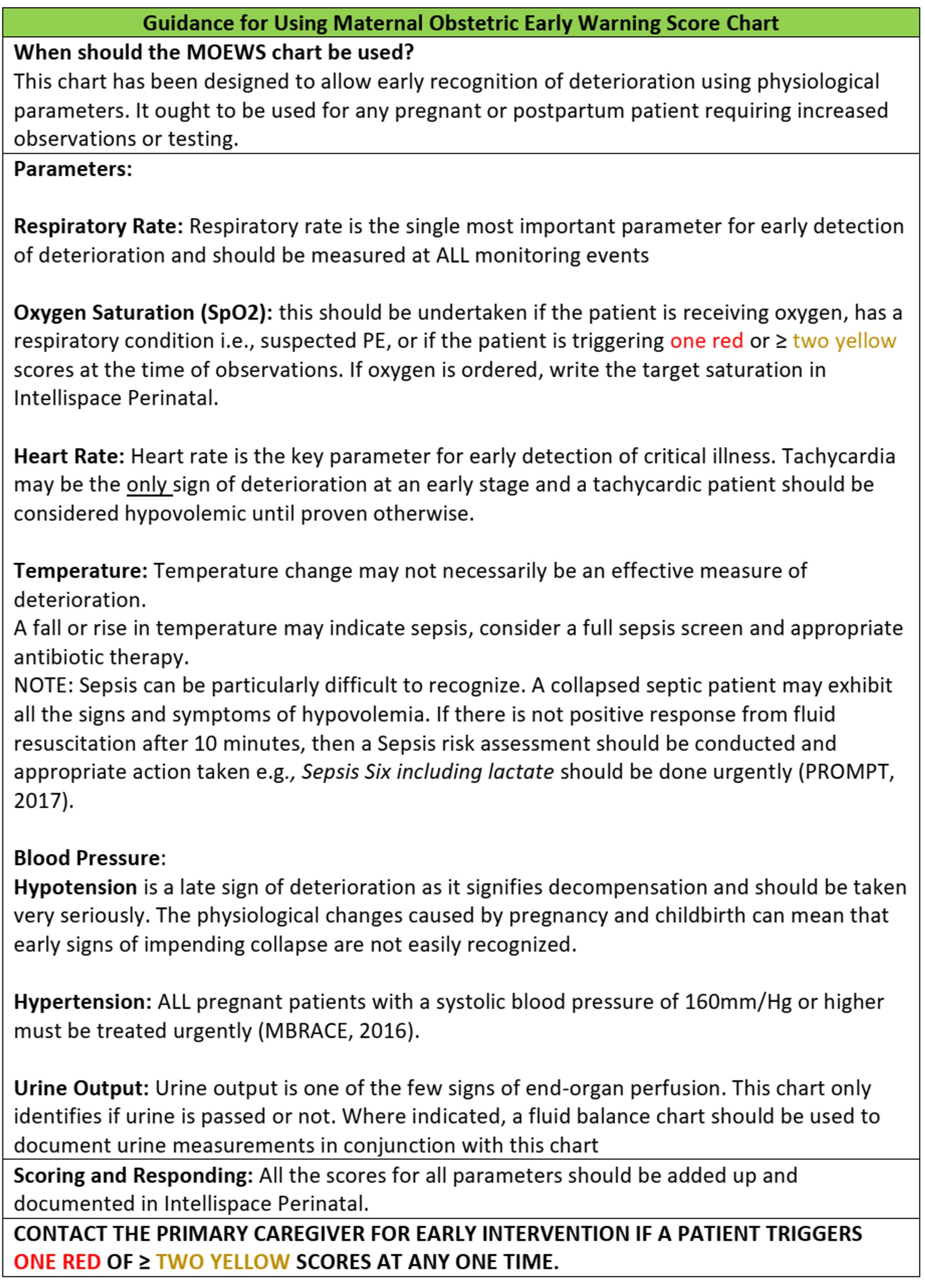
Risk stratification using MOEWS chart
Timely intiation of Sepsis Six care bundle: oxygen, cultures, antibiotics, fluids, lactate measurement and urine output monitoring
Broad-spectrum IV antibiotics within 1 hour of presentation for patients diagnosed with sepsis, ideally after blood cultures have been obtained
Multidisciplinary team approach and early critical care involvement
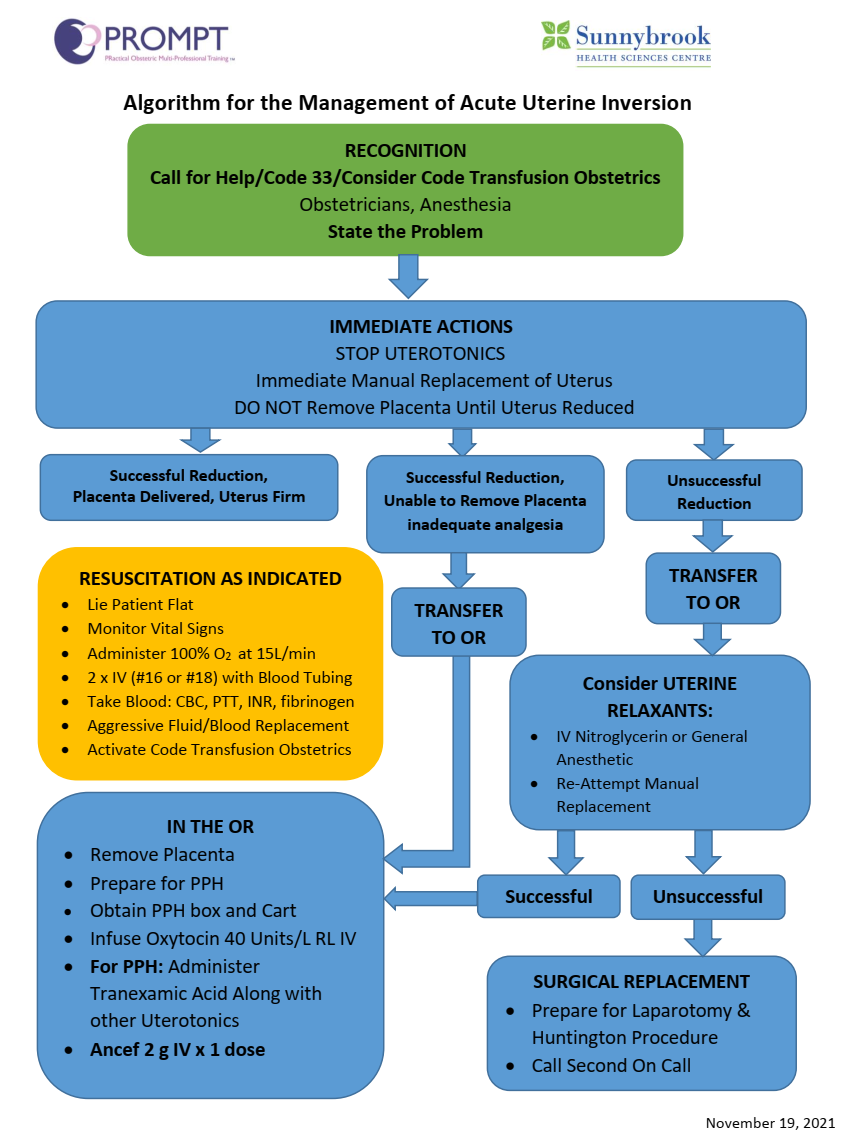
Uterine Inversion
True obstetrical emergency due to rapid blood loss
Call for help, activate Ob massive transfusion code
Management goals:
Ongoing hemodynamic / volume resuscitation
Uterine relaxation / tocolysis for successful manual re-position
Adequate analgesia for manual re-position
Quickly get full set of vitals BP, HR, SpO2, temperature
Do a focused hx including previous anesthetics, co-morbidities, meds, allergy
Do a focused cardiopulmonary exam and airway exam, GA is highly possible
Diagnose and treat at the same time
Clinical assessment of volume status / shock? level of consciousness, JVP, postural BP/ HR change, capillary refill, diminished urine output
100% O2, 2 large bore IVs, communicate with blood bank to have 4u of PRBC available, call for help
CBC, INR, PTT, fibrinogen
Quickly assess if any other causes of postpartum hemorrhage; tone, tissue, trauma, coagulopathy
Transport patient to OR for further management while keeping ongoing O2 and fluid resuscitation en-route
Tocolysis:
Terbutaline 0.25mg IV (could cause hypotension, exacerbation of shock)
Nitroglycerine 50ug IV boluses
Magnesium sulphate 4g IV (at least 10 mins for onset), gives slowly to avoid cardiovascular depression, monitor toxicity
Beta agonist e.g. ventolin
Volatile agents, therefore GA. Might consider as first line option
If there is epidural in-situ, could potentially use it for analgesia for manual reduction. But be very careful with hemodynamic collapse since these patients are volume depleted
Prudent to avoid using neuraxial for analgesia (does NOT relax uterus), instead IV opioid (e.g. morpine 2-4mg) can be used
If going for GA:
Call for help
RSI
Styletted tube ready
Ideally arterial line pre-induction but don’t spend too much time on getting one
Preoxygenate
Ketamine 1-1.5mg/kg
Succinylcholine 1.5mg/kg
Any volatile at MAC 0.8-1 balancing between uterine relaxation and cardiac depression
O2/N2O
Once reduced, should followed by uterotonics injection i.e. oxytocin 2-5u slow bolus & 20-40u oxytocin in 1000ml volume infusion, escalating to ergot, hemabate if necessary
If ongoing bleeding despite full treatment of uterotonics and correction of clotting factors including platelets, FFP, fibrinogen concentrate; and avoid acidosis or hypothermia
If utereus is appropriately contracted but still ongoing shock, consider retroperitoneal bleed which could be amenable to embolization by interventional radiology or surgical intervention
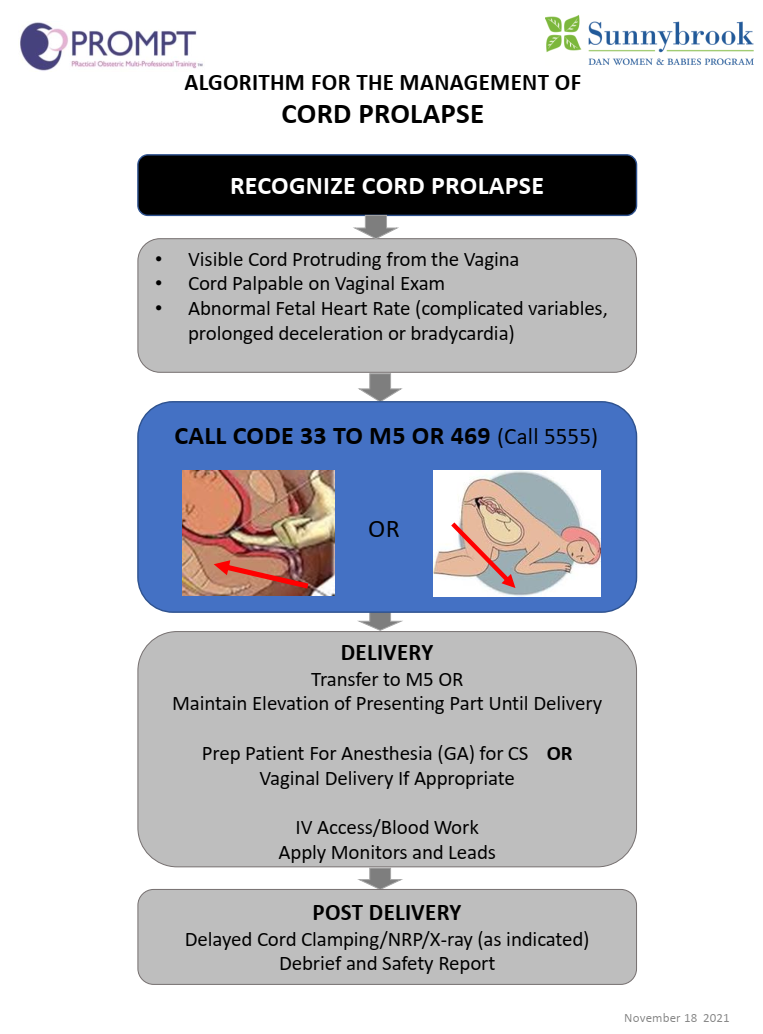
Umbilical Cord Prolapse
Obstetrical emergency requires prompt assessment, diagnosis and management
Overt prolapse (cord exits the cervix past the fetal presenting part & Occult prolapse (cords exits the cervix alongside the fetal presenting part)
Clinical diagnosis by palpation of a pulsating cord or a visible cord in the vagina (overt prolapse). For occult prolapse, only fetal bradycardia or sever variable decelerations is present
Risk factors:
Premature rupture of membran
Preterm delivery
Low birth weight
Polyhydramnios
Breech presentation
Multiple gestation
External cepahlic version
Management
Goal to avoid cord compression and umbilical vessels vasospasm that can lead to fetal hypoxia potentially causing fetal demise or permanent cerebral injury
Activate code obstetrics (code 33), call for help (Ob, Anesthesia, RT / AA, Neonatoloy, OR team)
Establish IV line, oxygen via face mask
Avoid aortocaval compression
Minimize handling of the cord to avoid vasospasm
Umbilical cord prolapse necessitates immediate delivery usually via emergent C-section, most likely under GA given the emergency
Keep the cord warm and moist if imminent delivery is not feasible
Tocolysis if delivery is expected to be delayed
Elevate fetal presenting part to help with cord (funic) decompression
manual elevation of fetal presenting part with fingers / hand
steep trendelenburg or knee-chest position
filling urinary bladder (500ml NS) with foley catheter
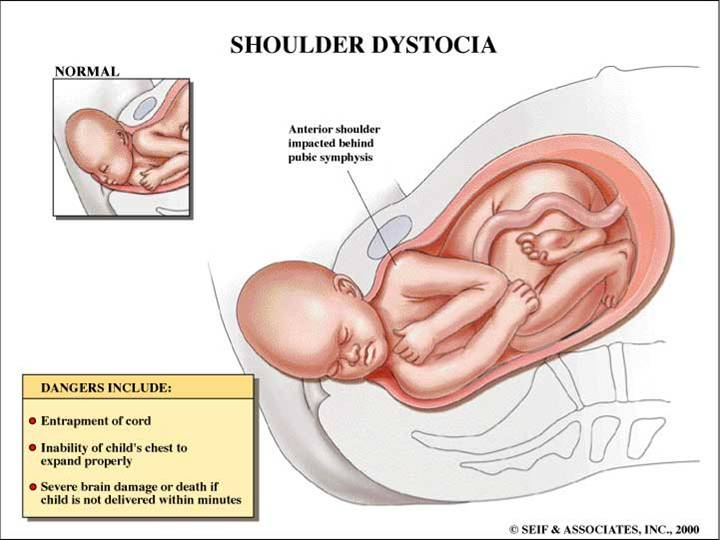
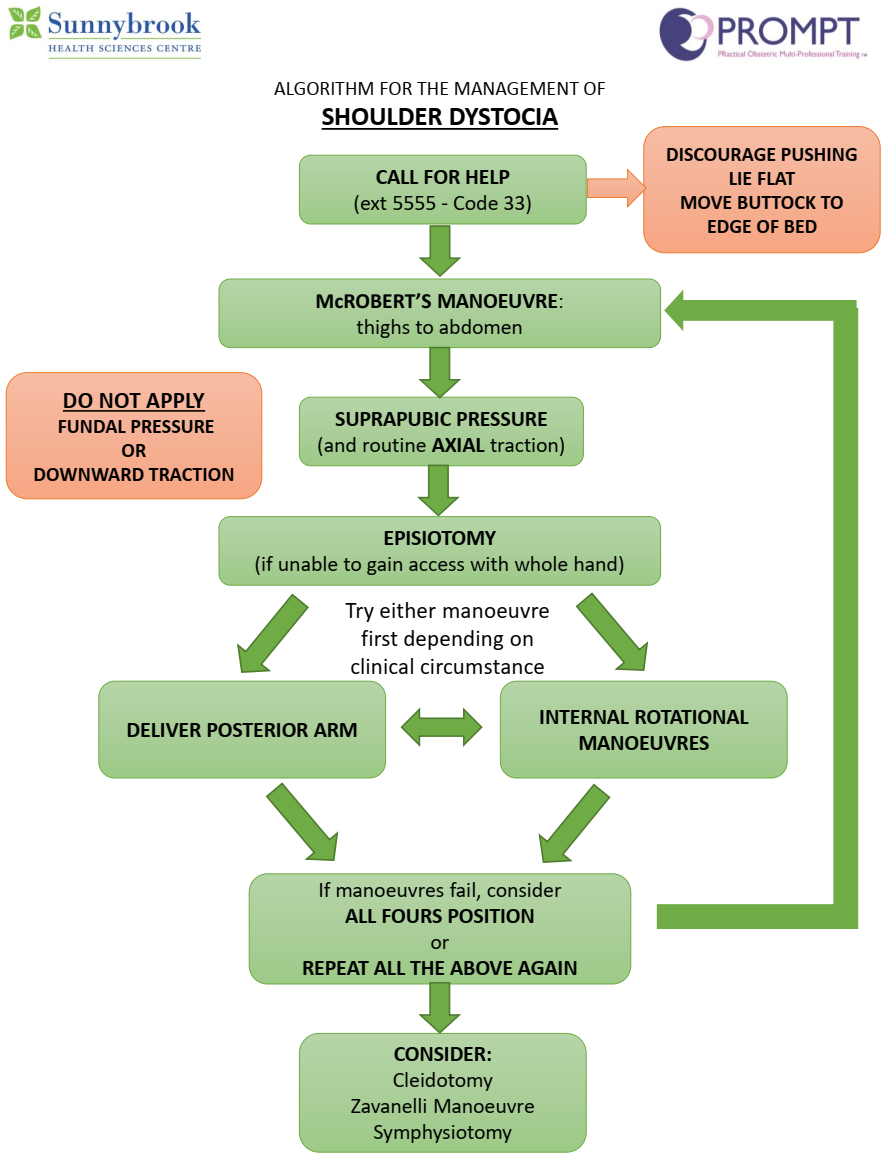
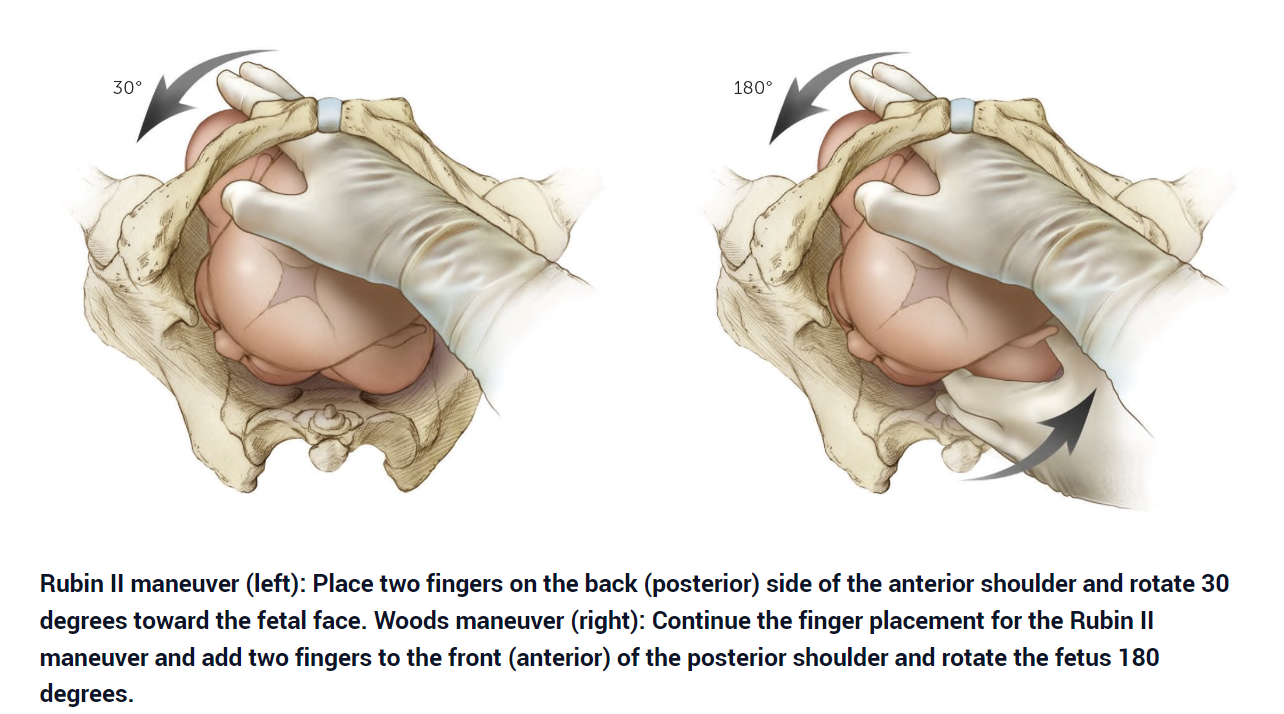
Shoulder Dystocia
An obstetric emergency requires timely management / delivery to minimize risk of fetal asphyxia
Descent of the fetal anterior shoulder is obstructed by the maternal pubic symphysis, or less commonly the fetal posterior shoulder is impacted on the maternal sacral promontory
Retraction of the delivered fetal head against the maternal perineum between pushes, i.e. “turtle sign.” This subtle sign can be an indication of shoulder dystocia
Risk factors
History of shoulder dystocia with previous deliveries
maternal diabetes, obesity
fetal macrosomia
prolonged second stage of labor
multiparity
BUT most cases of shoulder dystocia happen with normal sized babies and most vaginal deliveries with high birth weight do not result in shoulder dystocia i.e. shoulder dystocia occurs unpredictably
Management
Call for help, activate code obstetrics (code 33) - mobilize Anesthesia, AA / RT, Obstetrics, Nursing and Neonatology
Supplemental oxygen via face mask
If available, top up epidural to provide analgesia for management maneuvers
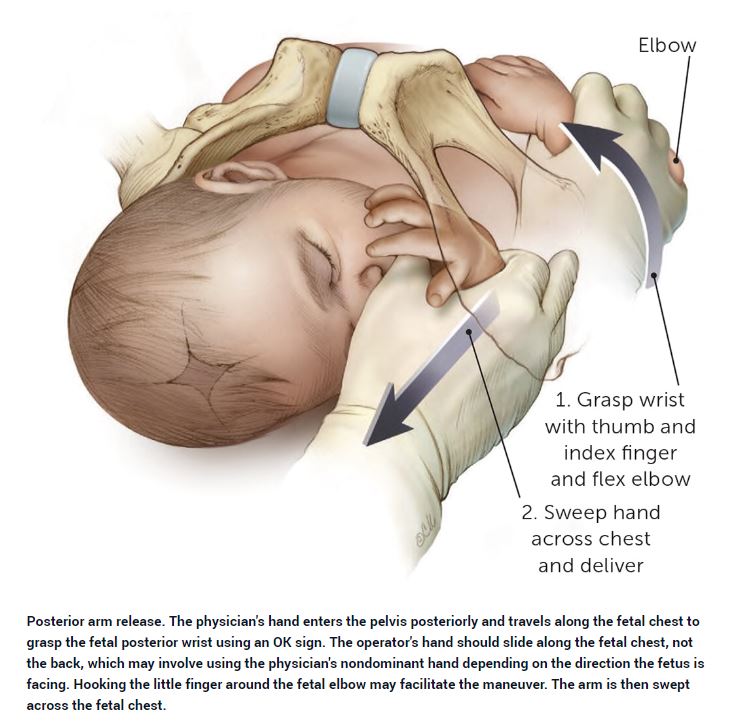
Goal of treatment is to perform maneuvers that increase the functional diameter of the pelvic ring, decrease the breadth of the fetal shoulders, or change the relationship of the breadth of the fetal shoulders within the pelvis
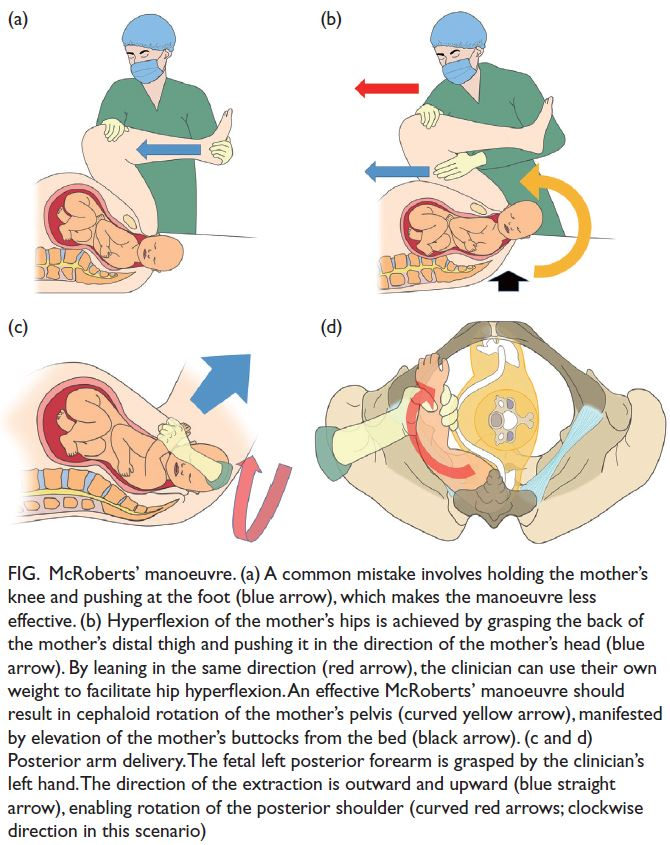
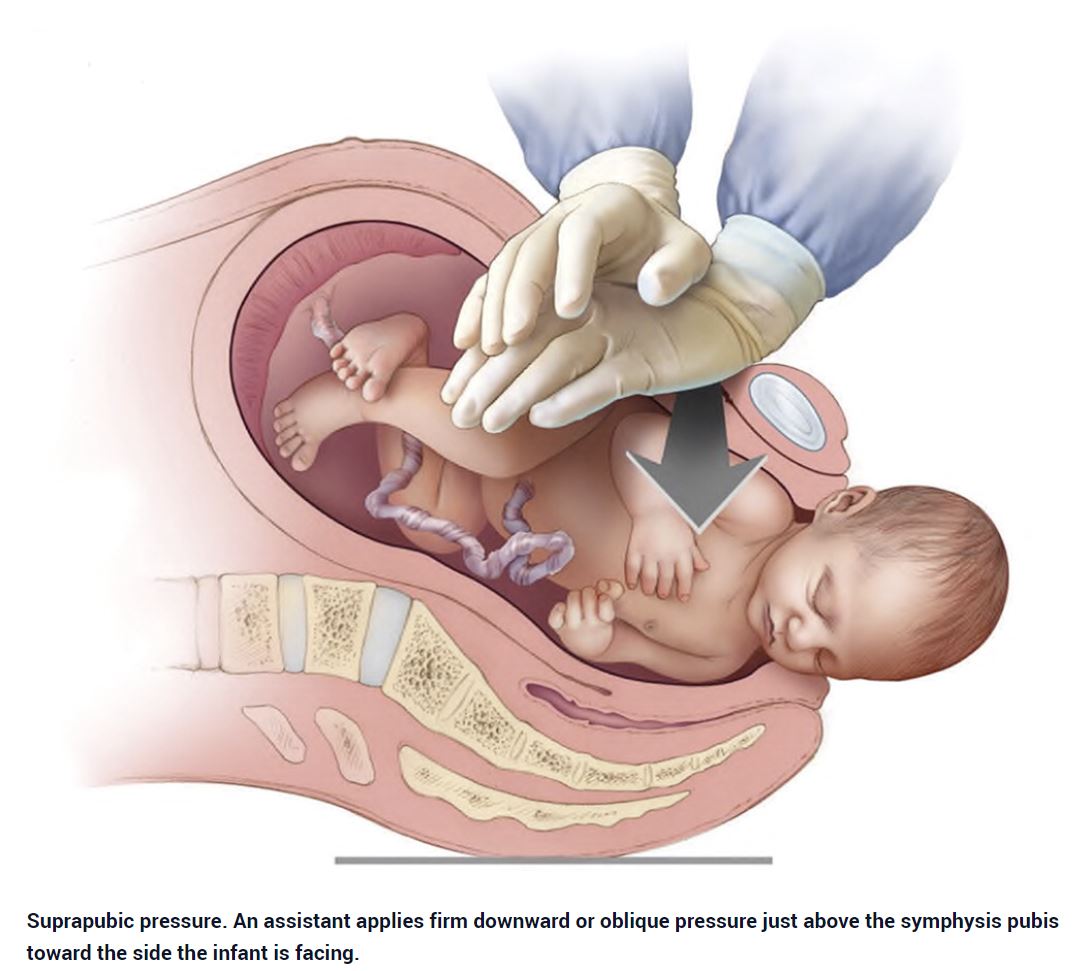
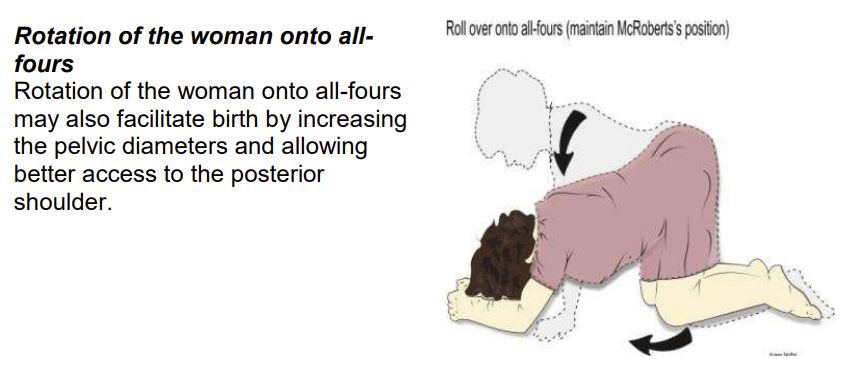
The pregnant woman should be instructed to stop pushing, move buttocks to end of the bed to aid management maneuvers e.g. McRoberts, suprapubic pressure
Amniotic Fluid Embolism
Emergent; call for help, activate code OB, notify ICU
Assess, diagnose and management simultaneously
Multisystem involvement:
Cardiovascular collapse, biventricular failure
Pulmonary edema, hypoxia
Altered mentation, LOC, seizure
DIC , coagulopathy
DDx:
Obstetrical:
Eclampsia
Abruptio placenta
Uterine rupture
Peripartum cardiomyopathy
Non-obstetrical:
PE
Myocardial infarction
Sepsis
Anaphylaxis
Venous air embolism
Iatrogenic:
High spinal
Local anesthetic systemic toxicity
Medication error
Establish definitive airway for adequate ventilaion & oxygenation, 100% oxygen
Central venous access for fluid resuscitation and/or intropes and pressors
Arterial line for hemodynamic montoring and frequent blood sampling
ACLS protocol with OB modification e.g. manual uterine displacement; on-scene peri-mortem cesarean section if no ROSC within 4 minutes of resuscitation
Treatments focus on increasing cardiac output and pulmonary vasodilation, decreasing right heart strain, and providing massive transfusion of blood products in case of DIC. Dobutamine, inhaled nitric oxide and inhaled prostacyclin are to be considered to assist with pulmonary vasodilation.
Contact blood bank for C1 esterase inhibitor (C1INH).
Multiple Gestations
Increases maternal issues:
Exaggerated aorto-caval compression, propensity to desaturation
PPROM
Preterm labor
Prolonged labor
Pre-eclampsia/eclampsia
Placental abruption
Operative delivery
Uterine atony
Antepartum & PPH
Fetal issues:
Premature delivery
IUGR
Twin-twin transfusion
Polyhydramnios
Cord entanglement
Umbilical cord prolapse
Malpresentation
Trial of labor & vaginal delivery
To be performed in OR with double setup in preparation for possible C-section
Adequate epidural analgesia
2 large bore IV's
Prepared for STAT C-section with GA
Diluted nitroglycerine available for uterine relaxation to facilitate internal version & breech extraction
NICU personnel present
Cesarean section
2 large bore IV's & cross matched
Modes of anesthesia - epidural, spinal, & GA depending on risks vs benefits
Be prepared for exaggerated aortocaval compression & rapid desaturation
Nitroglycerine ready for uterine relaxation
Be prepared for post partum hemorrhage, need for resuscitation & uterotonics
NICU personnel present
Trauma
Leading cause of non-obstetrical maternal mortality; non-lethal injuries 1 in 12 pregnant women
MVC, fall, domestic violence and other non-accidental causes etc. GSW, stabbing
Every female of reproductive age with significant injuries should be considered pregnant until proven otherwise
Emergent; assess, diagnose and manage simultaneously
Urgent Ob / neonatology consult especially at a viable age i.e. 23 weeks or older
Pregnancy considerations: two patients, aortocaval compression, full stomach, difficult airway, baseline compensated respiratory alkalosis etc.
Trauma considerations: multi-system involvement, hemodynamic instabilities, potential C-spine injury, potential facial / neck injuries impacting on airway management, chest injuries causing respiratory / hemodynamic compromise, full stomach, substance intoxication, possible TBI, hypothermia etc.
Standard trauma algorithm, assessment and resuscitation priorities regardless of pregnancy; maternal well-being takes precedence ⇒ maintain uteroplacental perfusion and avoid fetal hypoxia and acidosis
Early aggressive intravascular repletion and volume resuscitation in case of hypovolemic shock; vasopressor use could compromis placental perfusion
History:
AMPLE
Mechanism of injury
Past obstetrical history and course of the current pregnancy
Vaginal discharge / bleeding, abdominal pain, intensity / frequency of contraction, maternal perception of fetal movement
Physical Exam:
Follow standard ATLS primary, secondary and tertiary servey
Avoid aortocaval compression by left lateral tilt, manual displacement while supine or lateral tilt with backboard for spine precaution
Paying particular attention to physiologic change in pregnancy: reduction in FRC and increased minute ventilation ⇒ prone to desaturation, increased plasma volume by 50% leads to delayed recognition of hemorrhagic shock, baseline tachycardia 15-20 bpm elevation by 3rd trimester
Palpate uterus for fundal height, shape, hypertonus and tenderness
With viable fetus (23 weeks or older), cardiotocography or electronic fetal monitor for at least 4 hours
Ob to perform vaginal exam for cervical dilatation, effacement, fetal presentation / station; in case of vaginal bleeding, speculum or digital vaginal examination should be deferred until placenta previa is ruled out by U/S
Lab & Investigations:
Standard trauma panel; note normal pregnancy changes e.g. elevated WBC up to 20, dilutional anemia down to 100, reduction in creatinine, elevated ALP up to 140
Coagulation profile including fibrinogen; note normal increase in fibrinogen during pregnancy up to 4+
X-ray or CT studies as indicated for maternal evaluation and should not be deferred due to concerns regarding fetal exposure
FAST is equally sensitive and specific
Pregnancy specific concerns:
Placental abruption
Could happen in even minor trauma ⇒ maintain high index of suspicion
Can be triggered by placental abruption, PPROM etc.
Nitrazine paper or ferning test ?ROM
Fetal fibronectin test ?preterm labour
Systemic steroid for fetal lungs maturation and MgSO4 for neuro protection
Neonatology consultation
Amniotic fluid embolism
Rare
Catastrophic hemodynamic and respiratory collapse
Supportive maternal care
Expedited C-section delivery depending on gestational age
Prevention of Rh alloimmunization
Rh antigen is well developed by 6 weeks gestation
0.001ml of fetal blood can casue sensitization in Rh- mother
Anti-D IgG 300ug should be administered to all Rh- pregnant trauma patients within 72 hours on injury
KB test might be warranted to quantify amount of transplacental hemorrhage, if more than 30ml of fetal blood in maternal circulation, additional dose of anti-D IgG
Perimortem C-section
Within 4 min following maternal cardiac arrest while maintaining CPR / maternal resuscitation
Recommended for viable fetus at or older than 23 weeks or fundal height 2 or more fingerbreadths above umbilicus
Should be performed at the scene of cardiac arrest instead of transferring to OR
Chest tube placement - due to elevation of disphragm by gravid uterus, insertion sites should be 1-2 intercostal spaces higher to avoid intra-abdominal placement
Tetanus shot prn; safe during pregnancy
Non Ob Surgery During Pregnancy
1-2% of all pregnancy e.g. laparoscopic cholecystecomy, appendectomy
Pregnancy considerations
Latest 2019 April ACOG Committee Opinion
No currently used anesthetic agents have been shown to have any teratogenic effects in humans when using standard concentrations at any gestational age
A pregnant woman should never be denied medically necessary surgery or have that surgery delayed regardless of trimester
Pregnant women undergoing nonobstetric surgery should be screened for venous thromboembolism risk and should have the appropriate perioperative prophylaxis administered
Elective surgery should be delayed after delivery
Ob +/- neonatology consult
Goal to maintain uteroplacental perfusion; avoid hypotension, hypoxemia, acidosis
Avoid NSAIDs (aspirin, ibuprofen, naproxen, diclofenac, and celecoxib) at 20 weeks or later gestation; potential risk of causing fetal renal issue leading to oligohyraminos. NSAIDs at 30 weeks and later is also not recommended because of the additional risk of premature closure of the fetal ductus arteriosus. These recommendations do not apply to low dose (81 mg) aspirin for specific pregnancy-related conditions under the direction of a healthcare professional, or to NSAIDs administered directly to the eye.
Neuraxial technique generally preferred
If GA & mechanical ventilation, remember ABG during pregnancy (pH increases 7.4-7.47, PaCO2 decreases 30mmHg, PaO2 increases 105mmHg, HCO3- decreases 20mmol/L)
In previable fetus (< 24 weeks), FHR by doppler pre and post surgery is sufficient
For fetus > 24 weeks, FHR monitor & toco monitor pre and post surgery to ascertain fetal well being & sign of preterm labour. Introperative FHR monitor is rarely needed.
Risk of preterm labour - consider steroids (Celeston) for lung maturity & magnesium for brain protection
Surgical considerations of a gravid uterus e.g. trocar insetion
Neurosurgical Emergency
Timely multidisciplinary involvement i.e. neurosurgery, obstetrics, neonatology, anesthesiologists specialized in obsetrical / neuroanesthesia
Maternal considerations / well-being should take precedence in cases of emergent surgeries, irrespective of trimester
Paramount to minimize exacerbatioin of ICP, maintain cerebral & uteroplacental perfusion pressures
Keep in mind lower normal PaCO2 during pregnancy (≤ 32mmHg)
Goals to prevent secondary brain injury i.e. avoid hypoxemia, hypercarbia, hypotension, hyper / hypoglycemia, hyperthermia
Minimize contrast load and radiation during cerebral angiography e.g. single vessel angiogram, abdominal shield. Or consider MRA for initial evaluation
No evidence of mutagenic or teratogenic effects of iodinated contrast (category B i.e. no harm to animals, no human studies)
Previable fetus, doppler is sufficient for fetal HR monitoring; for viable fetus, cardiotocography should be performed (before and after the procedure or positioning e.g. prone)
For viable fetus with fetal pulmonary maturity, multidisciplinary decision regarding timing of delivery (mostly C-section) and surgical intervention i.e. before, after or concurrent
Delivery before surgical intervetion has the theoretical advantage of eliminating concern for adverse fetal outcome related to interventions during surgery e.g. hyperventilation, induced hypotension, mannitol use etc.
Neuraxial anesthesia is contraindicated in confirmed or suspected raised ICP
Also potential dural puncture with a large bore Tuohy needle with subsequent intracranial hypotension causing traction on the dura could result in rebleeding in certain cases
ICH
Aneurysm
More than 70% of ICH during pregnancy
Patients with known (intact) intracranial aneurysms, the risk of rupture during pregnancy and delivery is NOT increased; most (70%) patients will be delivered via elective C-section
However, ruptured aneurysm should be treated within 48 hrs of presentation; i.e. neurosurgical considerations should trump obstetrical consideration in ruptured aneurysms
Ruptured aneurysms more likely happen in 3rd trimester
Treatment modalities i.e. clipping vs coiling
Low dose mannitol (0.5 g/kg) has been used safely during pregnancy
During temporary clipping, induced hypertension (20% above baseline) and neuroprotective agents e.g. propofol boluses
AVM
About 20% of peripartum ICH
Increased risk of hemorrhage from pre-existing AVM during pregnancy (2nd & 3rd trimesters). Most would still recommend conservative management of unruptured AVMs in pregnant women
In cases of ruptured AVM, neurosurgical emergeny if herniation, acute hydrocephalus. Otherwise, need to balance fetal risk vs re-bleeding risk to decide whether to operate or expectant management. Case series has shown increased fetal and maternal mortality with conservative management
Treatment modalities i.e. endovascular +/- surgical resection
Tumors
Rare, no increased in frequency of brain tumors in pregnancy
Expenctant management in benign / asymptomatic growth
Malignant and / or symtomatic (mass effect) ⇒ surgical intervention
Anesthesia goals similar to non-pregnant patients while be mindful of maintaining uteroplacental perfusion & avoidance of aortocaval compression
TBI
Similar goals to non-pregnant patient, maintain uteroplacental perfusion and left uterine tilt
Avoid exacerbation of ICP i.e. head up 15-30 degrees, TIVA, avoid nitrous oxide, blunt hemodynamic response to intubation / pinning, avoid neck venous obstruction
In case of herniation, transient hyperventilation
Mannitol: pregnancy category B (no harm to animals, no human studies); hypertonic saline: pregnancy category C (no studies in animals or humans)
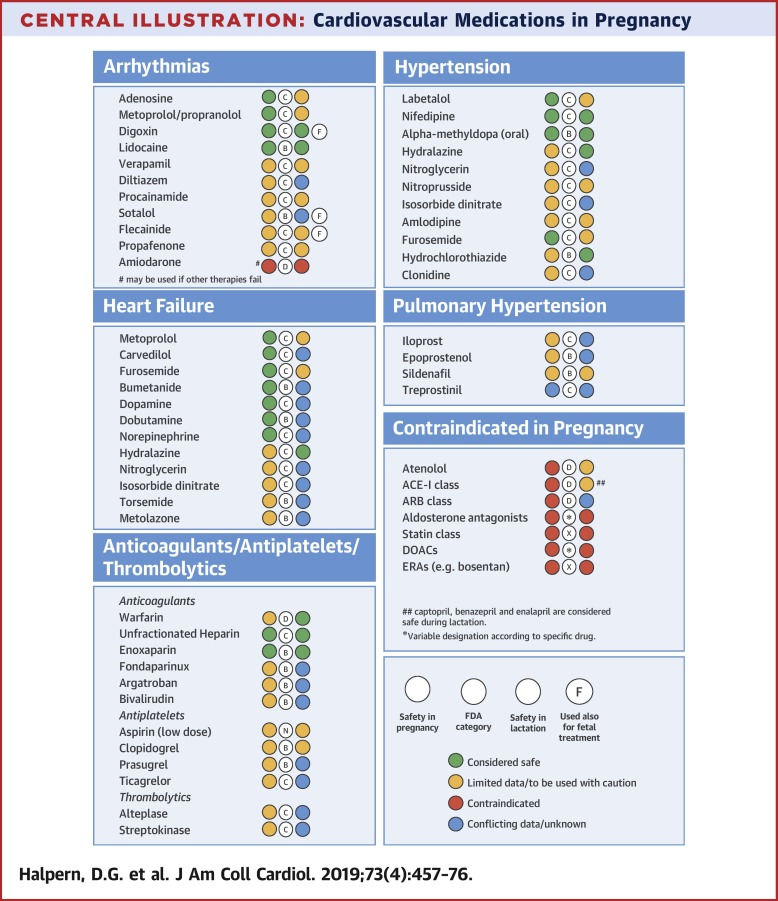
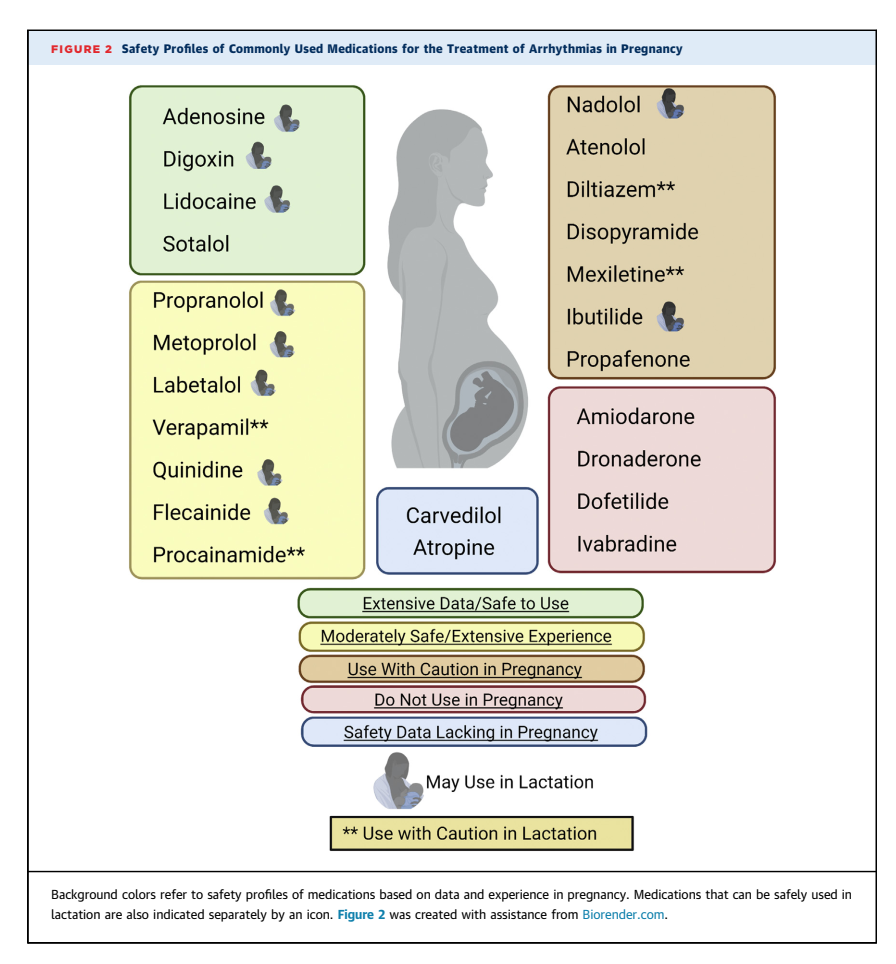
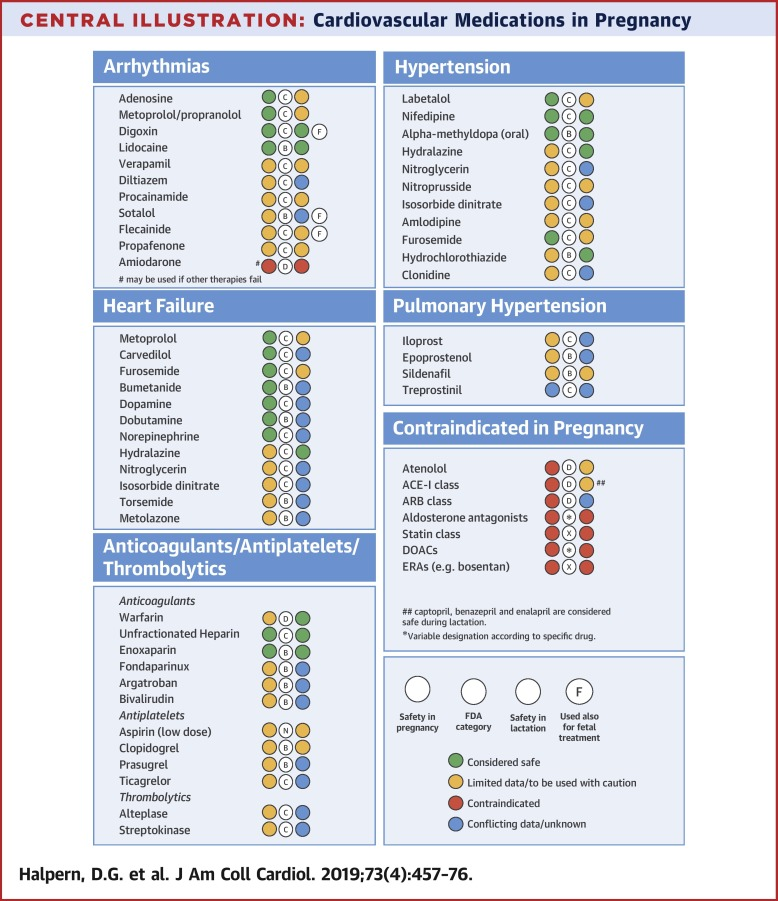
Arrhythmias During Pregnancy
Potentially urgent / emergent depending on hemodynamic stability and symptomatology
Even in stable patients, arrhythmias during pregnancy warrant timely assessment / diagnosis / management
History - cardiac symptoms e.g. dyspnea, SOBOE, chest pain / angina, PND, orthopnea, palpitation, syncope, presyncope; PMHx - CHD, structural heart disease, medication, past symptom; Family history of cardiac disease, sudden cardiac death
0.1% of all pregnancy-related admissions are associated with arrhythmia; but it is not uncommon for pregnant patients to experience palpitation or some form of arrhythmias during pregnancy, however, most do not require admission
Most frequent diagnosis sinus arrhythmia (60%), followed by atrial or ventricular extrasystole (19%) and paroxysmal supraventricular tachycardia (PSVT) (14%). Atrial fibrillation (AF) and atrial flutter (AFL) (1%), ventricular fibrillation (VF) (1%), and high-degree atrioventricular (AV) block (1%)
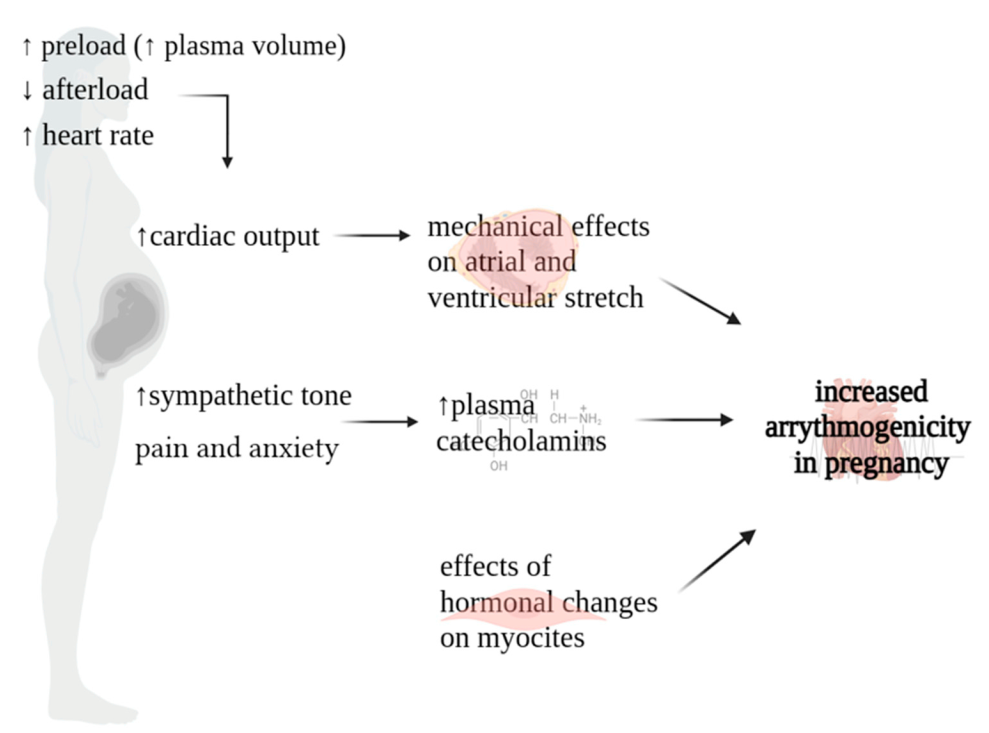
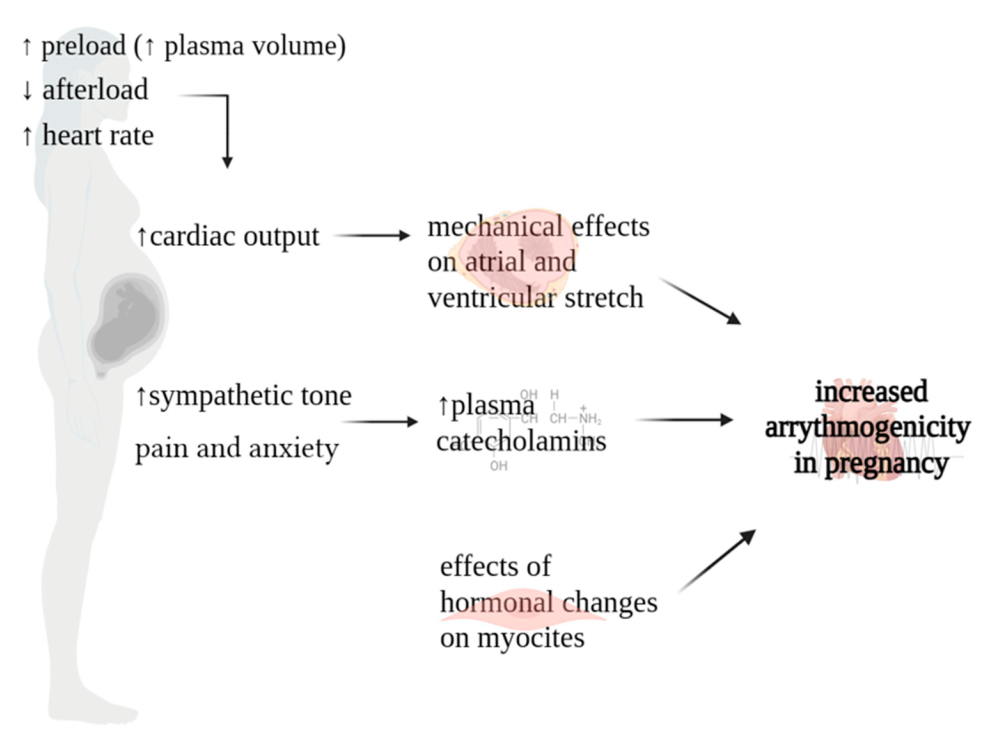
Pregnancy related hemodynamic, hormonal and autonomic changes promote arrhythmias during pregnancy especially in older patients and patients with congenital or structural heart diseases
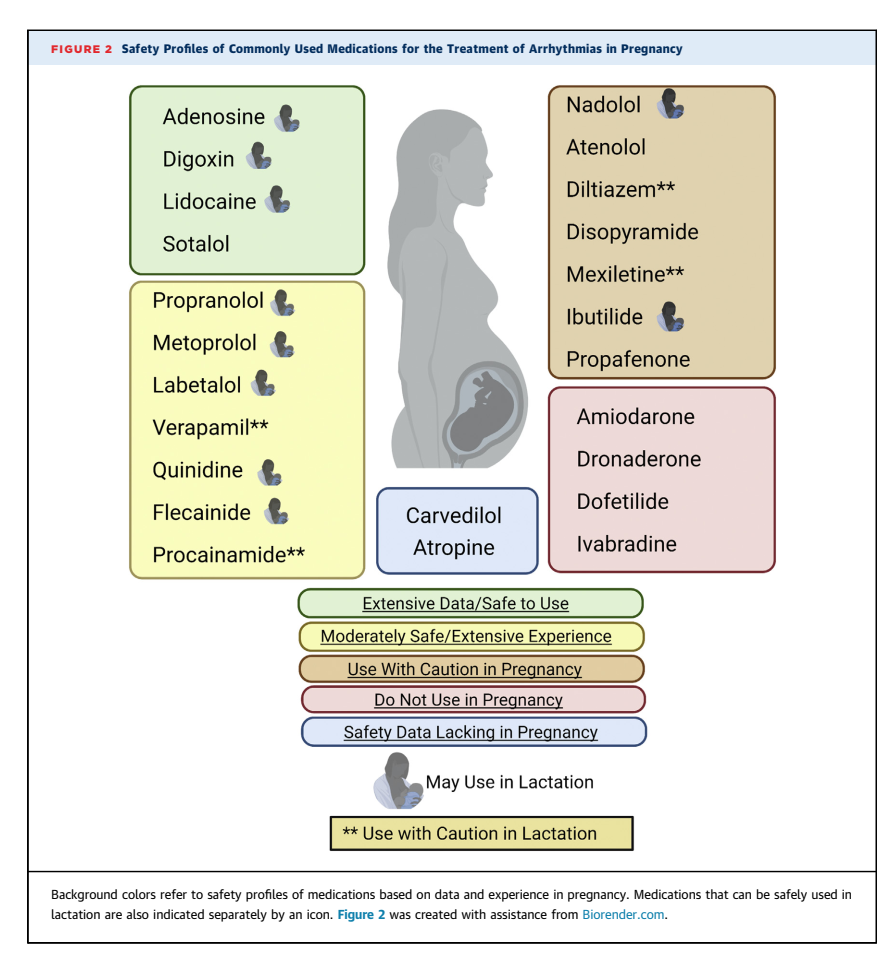
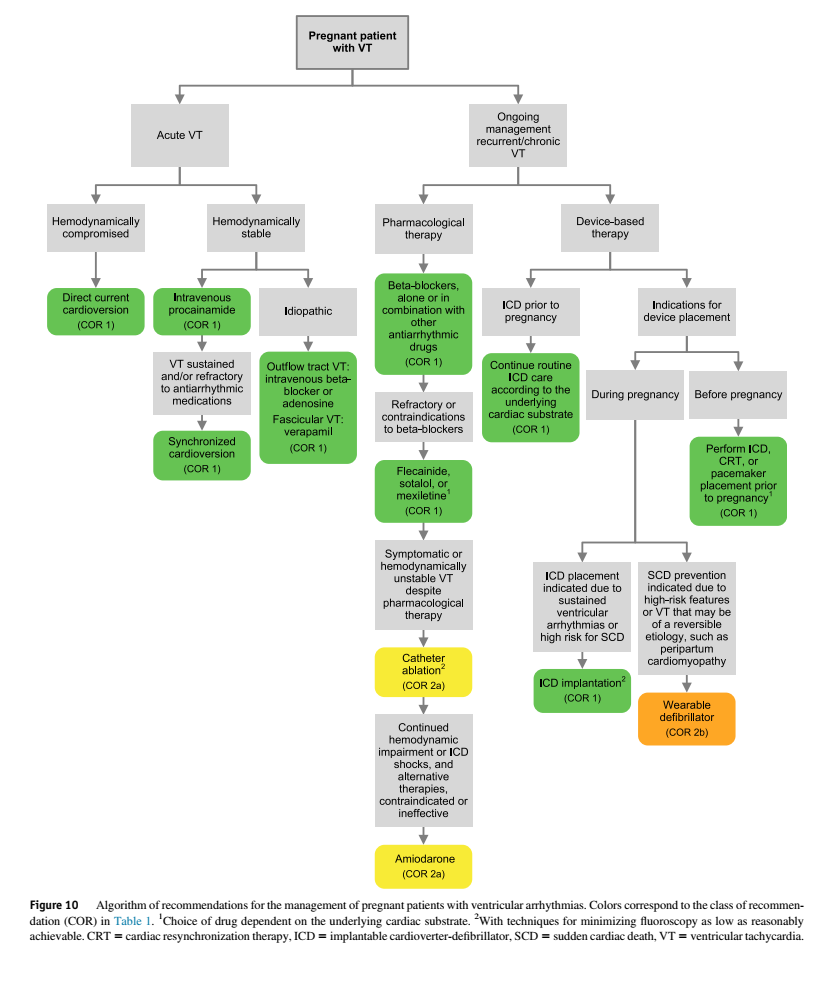
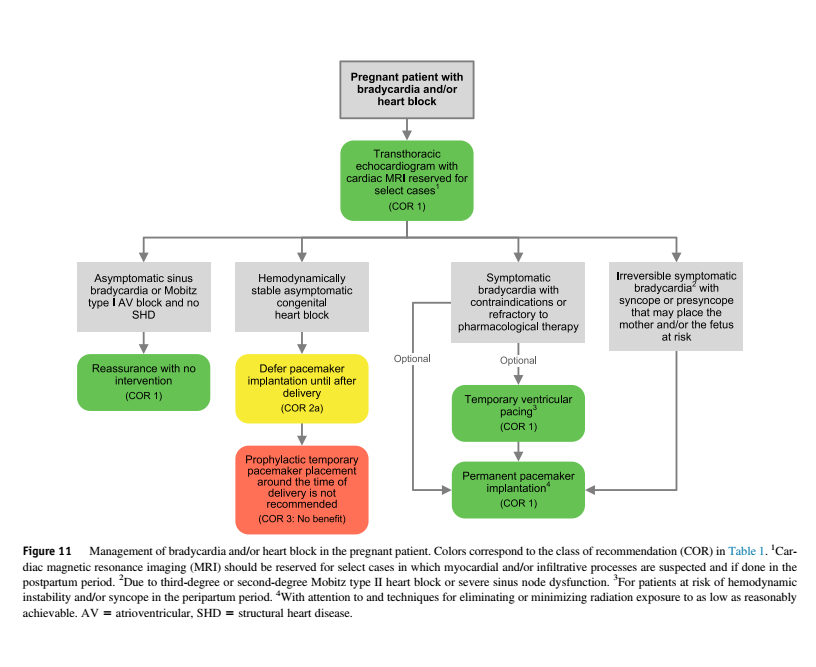
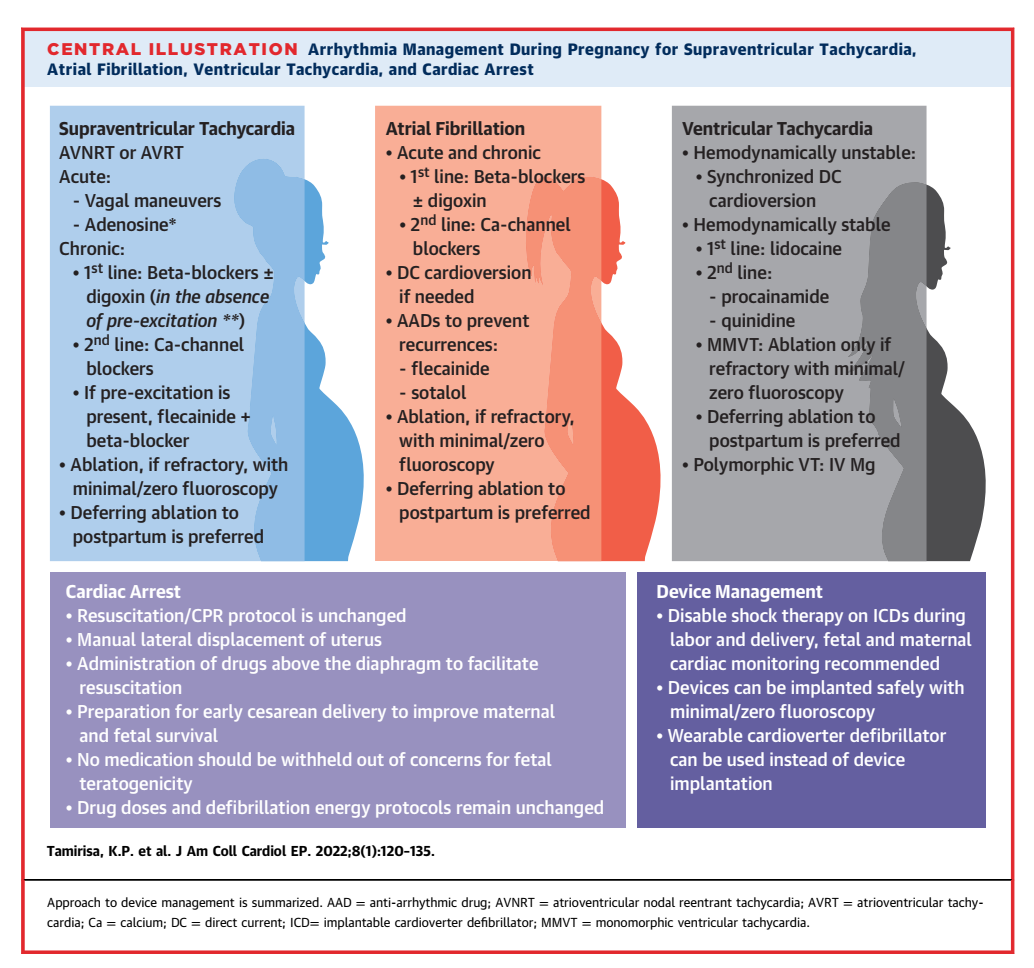
Approach to the treatment of arrhythmias in a pregnant patient is largely similar to the approach in a nonpregnant patient, but with modifications based on fetal safety e.g. drugs exposure, avoid radiation (PPM placement or cardiac ablation), left uterine tilt and shared decision-making among care team i.e. Ob, cardio-obstetrics, electrophysiology, neonatology, anesthesia
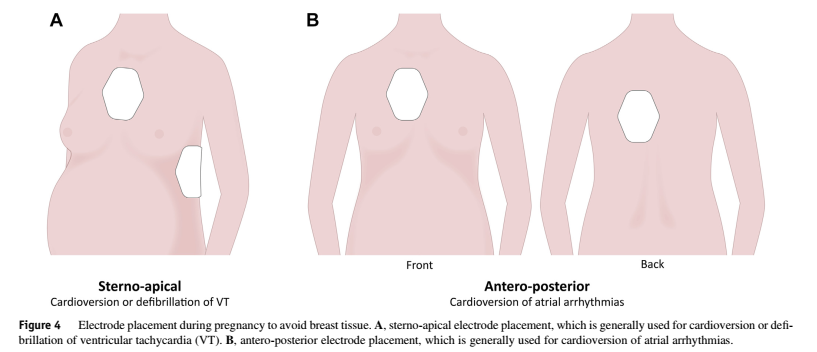
In pregnant patients with unstable SVT or VT, direct current synchronized cardioversion or defibrillation is recommended with energy dosing as in the nonpregnant patient. Electrodes should be placed to avoid breast tissues to optimize current delivery to the heart.
In pregnant patients with hemodynamically significant sustained cardiac arrhythmias refractory or with contraindications to pharmacological therapy who are candidates for catheter ablation, the benefit of controlling maternal tachycardia should be prioritized over the potential radiation risks to the fetus, especially if the procedure is done after the first trimester and radiation exposure is minimized to as low as reasonably achievable. In many cases, ablation can be performed without fluoroscopy.
In pregnant patients with cardiac arrhythmias, the route of delivery (vaginal or caesarean) should be determined by the birth plan and obstetrical factors in accordance with best clinical practice, along with continuation of antiarrhythmic drug therapy.
Adequate pain control during labor, ideally with the use of neuraxial / epidural anesthesia, to avoid pain-induced catecholamine surges that may exacerbate arrhythmias
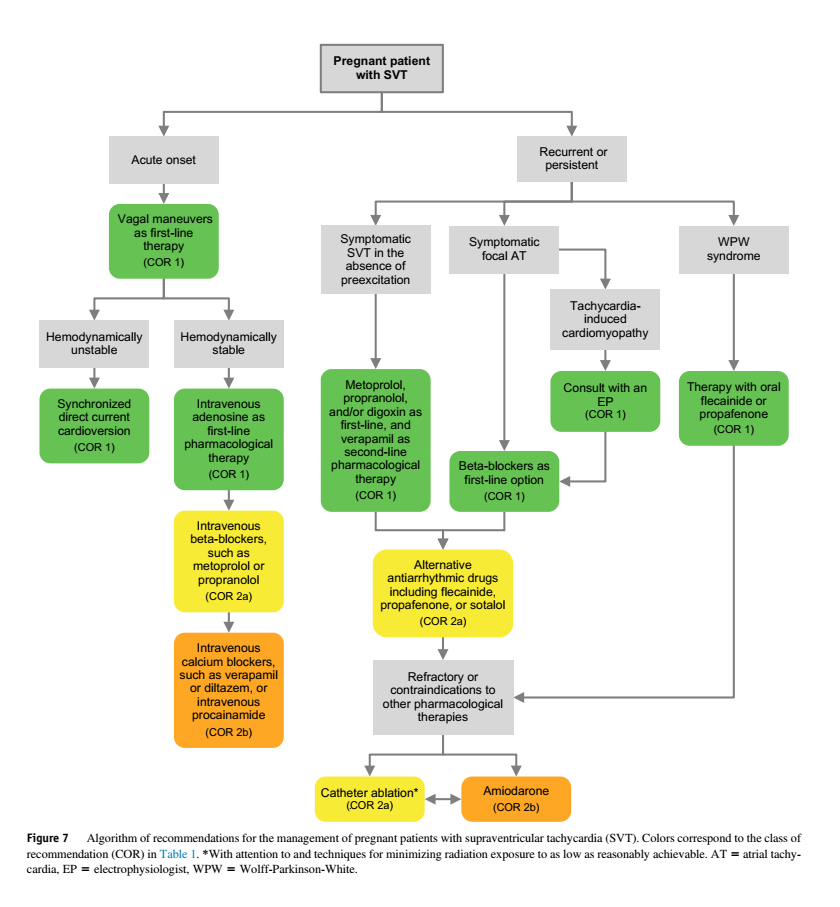
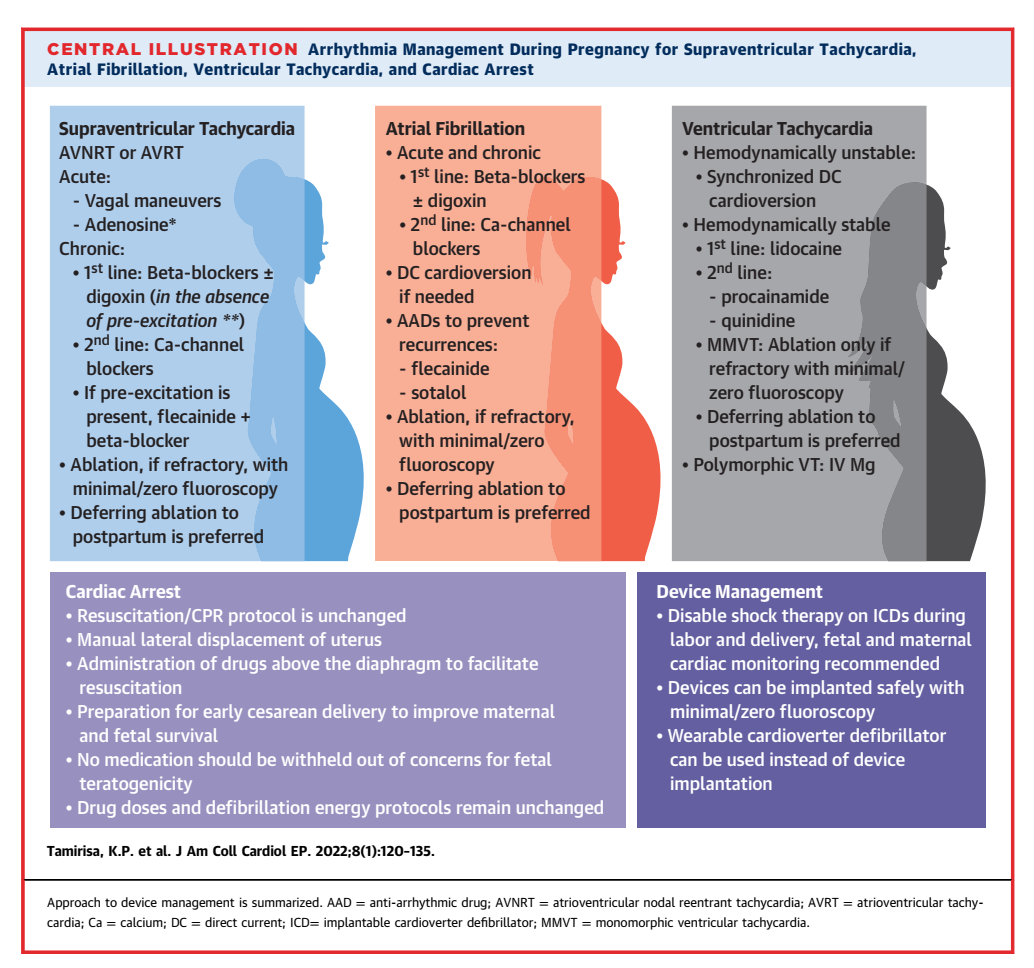
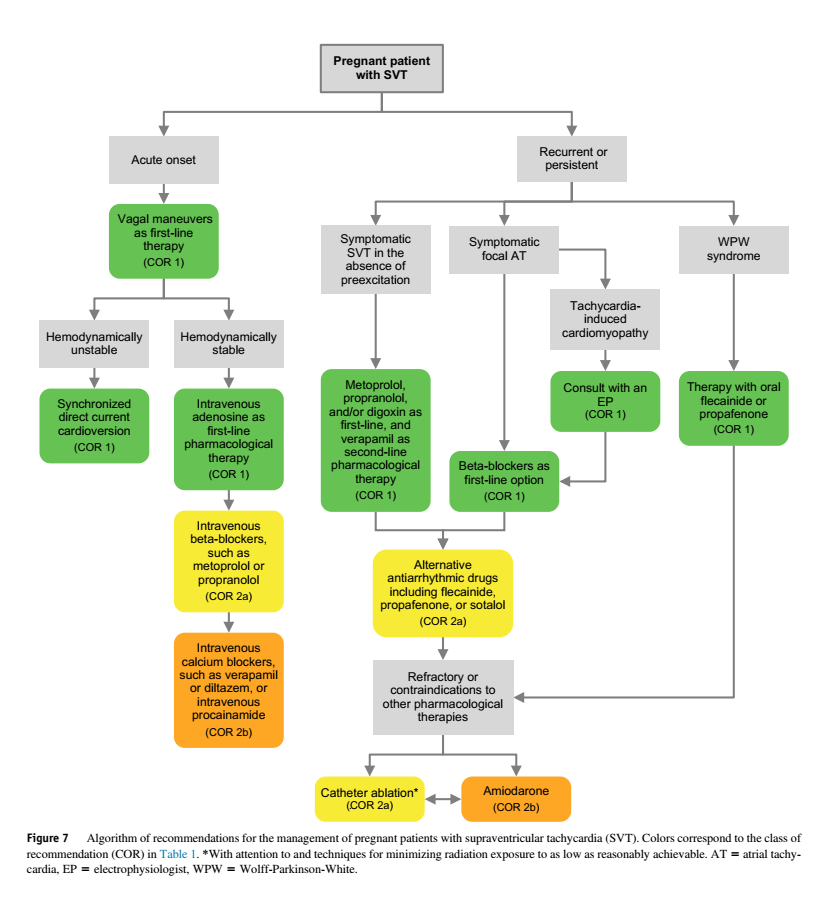
PSVT
In pregnant patients with acute onset of SVT, vagal maneuvers are recommended as first-line therapy for tachycardia termination.
In hemodynamically stable pregnant patients with acute onset of SVT, intravenous adenosine is recommended as the first-line pharmacological therapy.
In hemodynamically unstable pregnant patients with acute onset of SVT, synchronized direct current cardioversion is recommended, with energy dosing as in the nonpregnant patient.
In hemodynamically stable pregnant patients with acute onset of SVT refractory or with contraindications to adenosine, intravenous beta-blockers, such as metoprolol or propranolol, are reasonable for termination of acute SVT.
In hemodynamically stable pregnant patients with acute onset of SVT refractory or with contraindications to adenosine or beta-blockers, intravenous calcium channel blockers, such as verapamil or diltiazem, or intravenous procainamide may be considered.
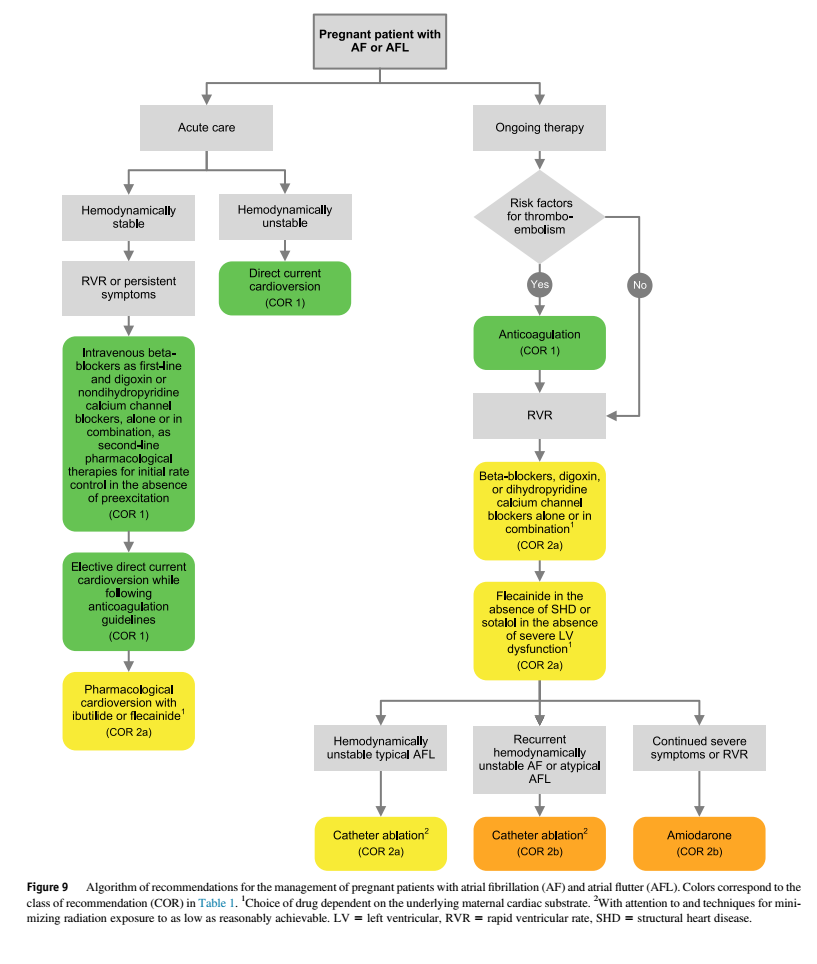
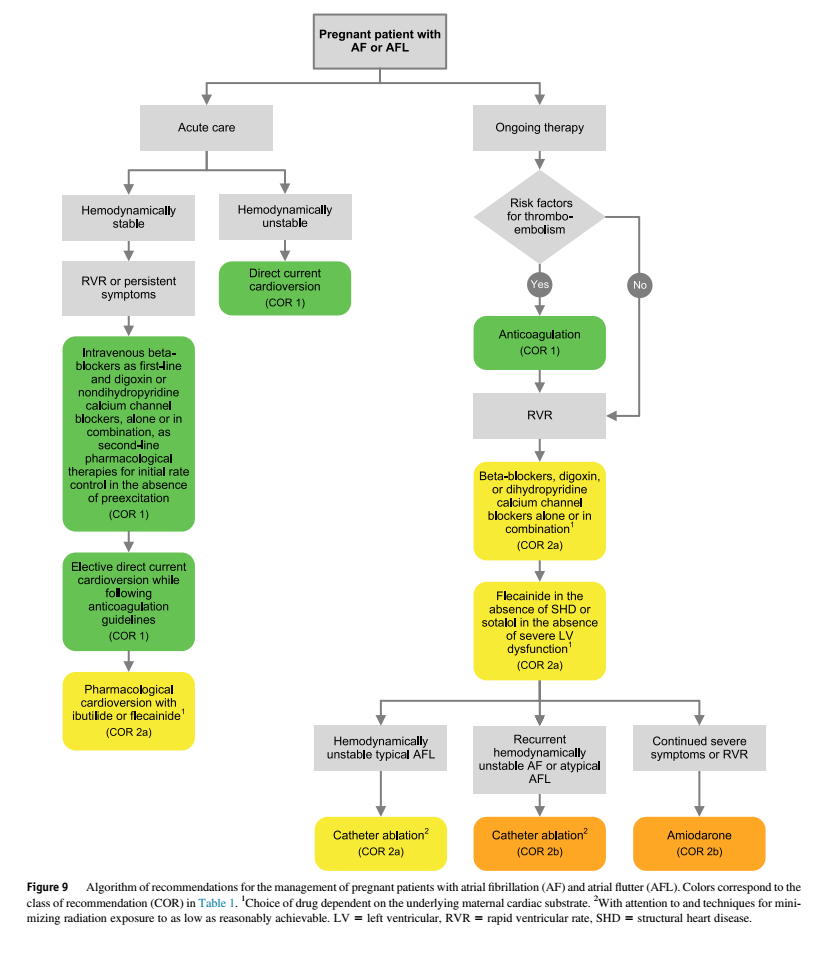
Atrial Fibrillation / Flutter
Unstable hemodynamics, direct current cardioversion is recommended, with energy dosing as in the nonpregnant patient.
Hemodynamically stable pregnant patients with AF or AFL with rapid ventricular rates, intravenous beta-blockers are recommended as the first-line option and digoxin or nondihydropyridine calcium channel blockers, alone or in combination, are recommended as second-line options for initial rate control
Persistent symptoms or rapid ventricular rate refractory or with contraindications to beta-blockers or calcium channel blockers, elective direct current cardioversion is recommended with anticoagulation with LMWH (Warfarin [>5mg] & DOAC are contraindicated during pregnancy) as in nonpregnant patients.
In pregnant patients with AFib or AFlutter and additional risk factors that place them at high risk for thromboembolism, anticoagulation is recommended as in the nonpregnant patient.
Recurrent hemodynamically unstable AFib or atypical AFlutter in whom pharmacological therapy is ineffective or contraindicated, catheter ablation may be considered with attention to and techniques for eliminating or minimizing radiation exposure to as low as reasonably achievable.
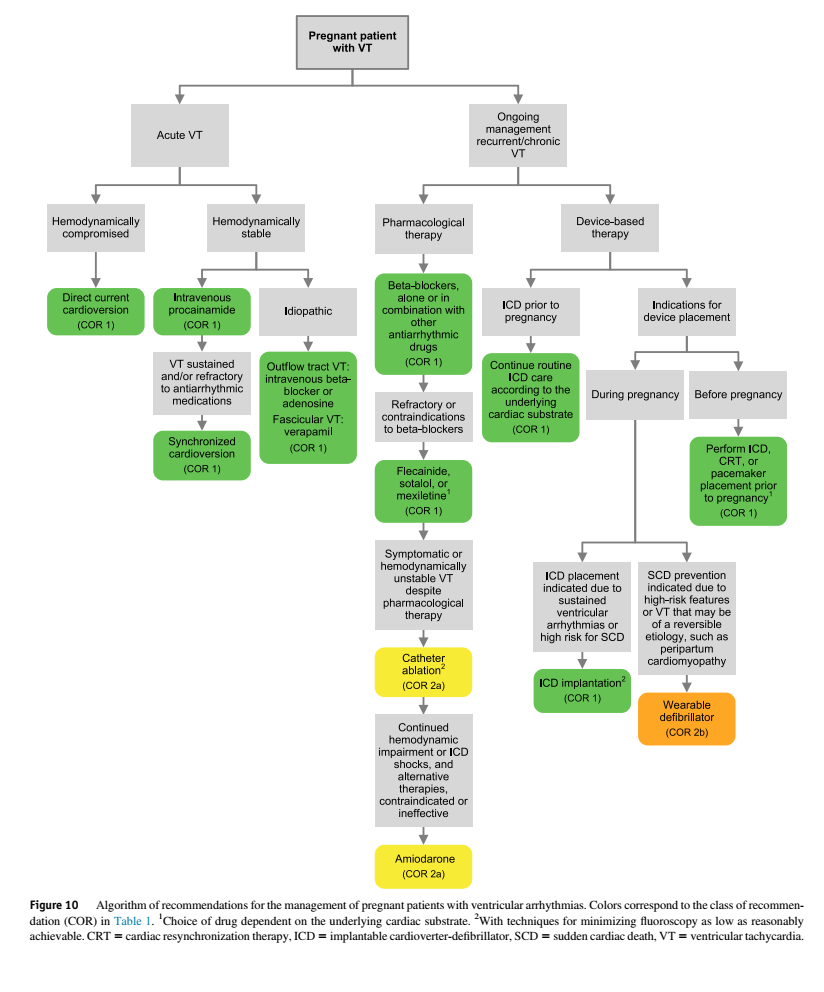
V Tach
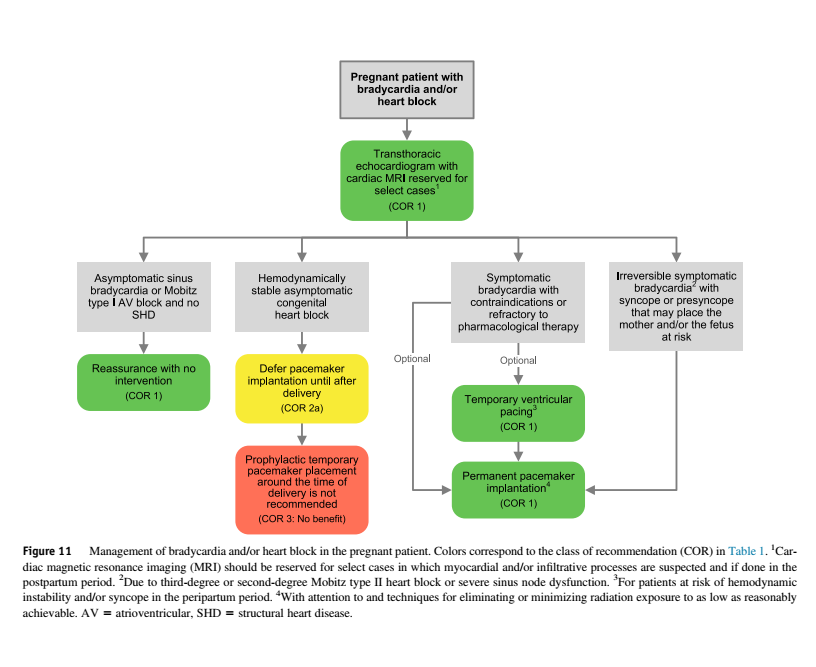
Bradycardia / Heart Block
Summary
Cardiac Arrest
Recommended ACLS chest compression technique and defibrillation protocol is no different from the non-pregnant guidelines
Epinephrine is preferred over vasopressin. Otherwise, ACLS drugs, including amiodarone, should be administered without modification
BLS and ACLS with following caveats / modifications:
Gestation age > 20 weeks or uterine fundal height above umbilicus ⇒ pulseless pregnant patient should be placed in supine position with manual left uterine displacement maneuver
NICU team should be involved without delay
Perimortem cesarean delivery should be initiated after four to five minutes from the onset of cardiac arrest at the location that the arrest occurred
Intravenous access should be obtained above the diaphragm if possible
If a fetal scalp electrode is present, this should be removed prior to defibrillation if possible

No Comments