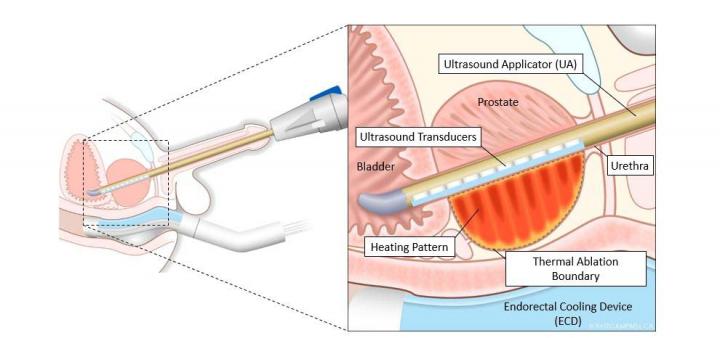
Transurethral Ultrasound Ablation (TULSA) for prostate CA. An outpatient procedure performed at research MRI (SG 23) on Friday. 1-2 patients, each case lasts for about 3-4 hours, or longer. Duration is dependent on prostate size and amount of calcification.
All cases at Sunnybrook have been done under GA (TIVA) with endotracheal intubation. Some centers have used spinal anesthesia. Given somewhat unpredictable duration and paramount importance of immobility during treatment, GA with paralytics is our default choice.
Note that patients have pre-treatment bowel preparation, be mindful about possible dehydration.
Marlene Kebabdjian (Dr. Klotz's assistant) will provide most of the equipments (e.g. ventilator circuit) and drugs (e.g. 100ml Propofol, Buscopan, Rocuronium). Stuff to bring with you:
Laryngoscope or Glidescope
Opioids, benzodiazepines
iPad for charting; note that vitals are to be charted manually on iPro
Ben Leung from Profound Medical (equipment vendor) will be onsite. He is a good resource for information about the procedure.
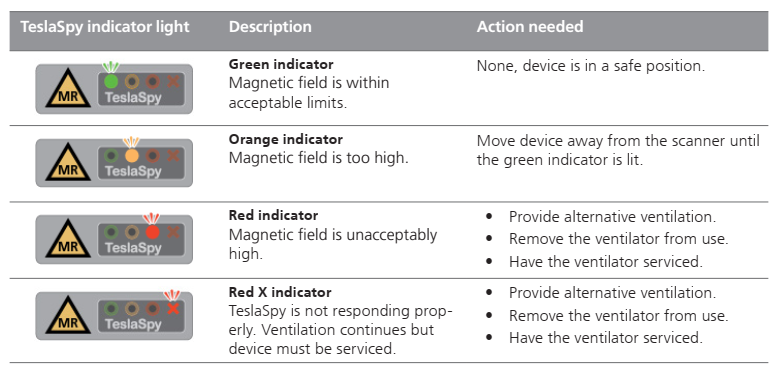
MRI conditional ventilator (Hamilton MR1) is located onsite. A quick guide is appended to the bottom of this page.
Caution: Do NOT move the ventilator too close to the MRI scanner. Pay attention to the magnetic field indicator light on the ventilator (bottom left). The ventilator needs to be serviced if red indicator is lit.
5 mirobore infusion tubings (5x2=10mL total priming volume) connected to provide adequate reach for TIVA. Tip: keep the tubings paper ties in place (except the one closest to the syringe pump) to avoid a tangled mess. Once passed into the MRI room through the conduit, uncurl the tubing one at a time. Note that the microbore tubing with 0.3ml priming volume will NOT work; injection pressure would be too high for the pump when there are five of those lines connected in series.
Or a single 25' minibore tubing (10ml priming volume) [see picture below] is availabe, ask Ruby.
Patient is positioned on the mobile MRI table outside the MRI room, then proceed with induction and intubation.
Urethra is cannulated with the ultrasound applicator in the MRI room. A series of MRI images will then be taken during the planning phase.
Prior to the treatment phase, patient's oral temperature is measured for software calibration purpose. Note that the digital thermometer is ferromagnetic! Hold on to it! It is a bit of work to fish it out from the core.
Suggest re-dosing paralytic prior to treatment phase. Patient's movement will necessitate re-planning. Also, a dose of IV Hyoscine (Buscopan) 20mg is given to minimize peristalsis. Dexamethasone and Ketorolac are also given to reduce post treatment prostate swelling.
Treatment causes mild (~20mmHg) but noticeable BP / HR rise; not enough to warrant use of fentanyl unless treatment phase is prolonged. There is no residual pain after treatment.
After treatment, ultrasound applicator removed and an indwelling urinary catheter is inserted prior to moving patient out of MRI room.
Patient is then transferred to a stretcher for extubation.
Disposition: M2 PACU then Same Day Surgery
Billing: The procedure is not covered by OHIP. Submit the billing card to billing office, an invoice will be issued to Urology for reimbursement. Our payment is time based, so document start and end time.




No Comments