
Renal Denervation (RDN) - Quick Guide
Background Info
-
Performed in Cath Lab #3 (across from C3, CICU).
-
As of the end of June 2024, Sunnybrook has done 6 cases. On average, RDN sessions are carried out once every 2 months.
-
Dr. Mina Madan (Cardiology) is the MRP with Dr. Andrew Dueck (Vascular Surgery) assisting. Feel free to contact Mina for any question regarding the procedure.
-
Mode of anesthesia - default is deep sedation and analgesia, very painful during radiofrequency ablation / denervation. Out of the 6 cases, 2 required conversion to GA (case #1 morbidly obese BMI 47, very anxious and likely difficult airway, reqiring esclataing dose of sedation / anaglesia; case #2 significant inspiratory diaphramatic excursion causing exaggerated descent of kidneys during ablation, hence GA with ETT for apnea during ablation).
-
Secondary causes of hypertension e.g. Cushing, Hyperaldosteronism, Pheochromocytoma would have been ruled out preoperatively.
-
End organ damage e.g. coronary artery disease would have been worked up by the cardiologist in some cases.
-
Be mindful about co-morbidities / metabolic syndrome e.g. obesity, diabetes, OSA, dyslipidemia.
-
All patients would have CT Angiogram preoperativley to assess for candidacy of RDN.
-
Immobility especially during ablation (each lasts for 60 seconds) is crucial for stability of the ablation catheter and success.
-
Both kidneys will be treated with total number of ablations varies depending on renal arteries anatomy and number of branches and accessory vessels, averaging 10+ ablations per session.
-
Each case takes about 2-3 hours.
-
Patients will be transferred back to CICU post procedure for recovery. Generally, no need for PACU even with GA.
Anesthesia Equipment
-
Anesthesia machine with iPad and drug cart is fully set up for GA but not frequently used, so budget extra time at the beginning of the day to check the cart and machine.
-
Bring your own opioids / benzodiazepines.
-
There is NO syringe pump, so call AA assistant (63134 or 88171) for 2 pumps ahead of time.
-
Set up own IV line with 2 three-way stop cocks at the distal end (for maintenance infusion), patients generally arrive with a 20G IV saline lock in-situ.
-
Glidescope and blades are located inside the cath lab control room.
-
Rt femoral artery accessed by cardiologist, arterial BP can be transduced and shown on their monitor.
-
Cardiology has an ultrasound machine in the room if one is neeed.
-
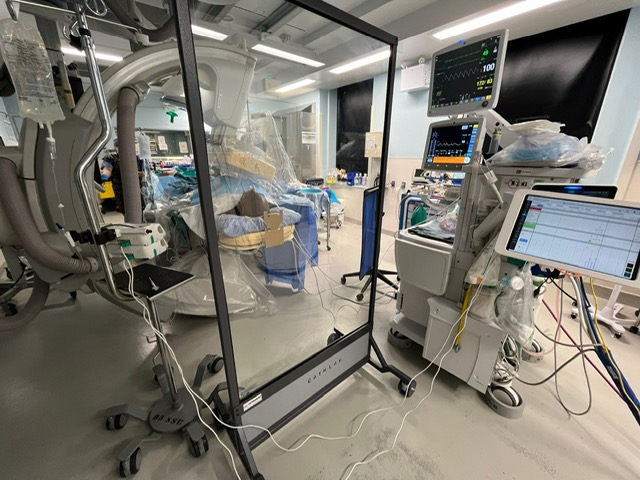
C-arm fluroscopy is used throughout, you will need lead apron and shield.
-
A typical setup as shown:
Tips
-
NO antibiotics required.
-
Heparin can be given IV by anesthesiologist or IA by the cardiologist. ACT is not generally checked.
-
Often intraarterial nitroglycerin will be administered by the cardiologist to alleviate renal arteries spasm, watch out for transient hypotension.
-
Possiblility of vasovagal response during ablation, so have treatment e.g. Atropin / Glycopyrrlate readily available.
-
Dexmedetomidine, Remifentanil, +/- Propofol infusion has been used successfully.
-
No flexion of hips for several hours post procedure given femoral artery puncture.
-
OHIP Billing Code J066, 6 units
Further Reading
-
Indications: refractory hypertension, intolerant to pharmacological intervention.
-
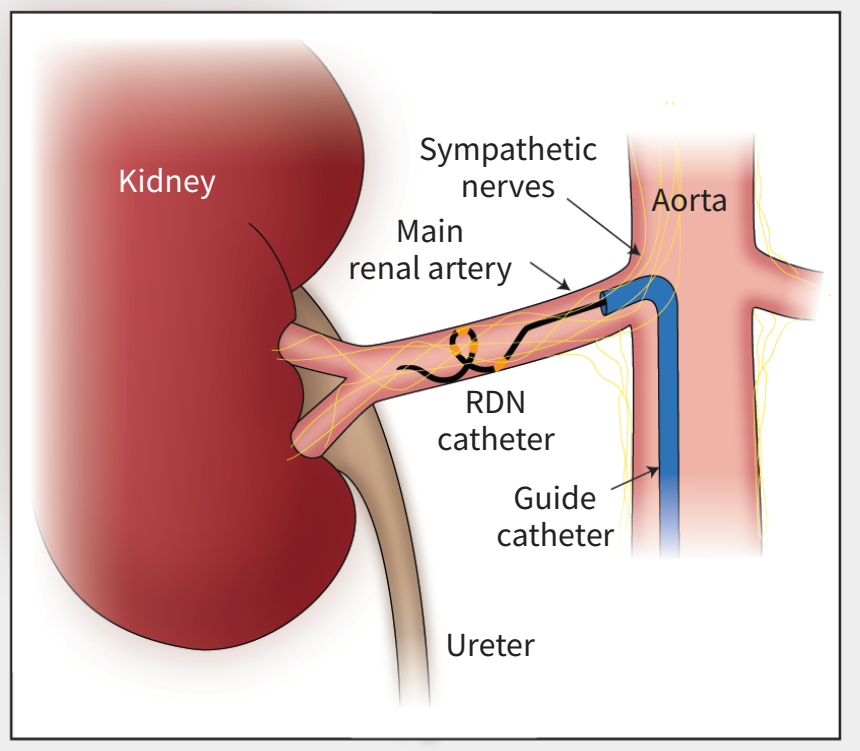
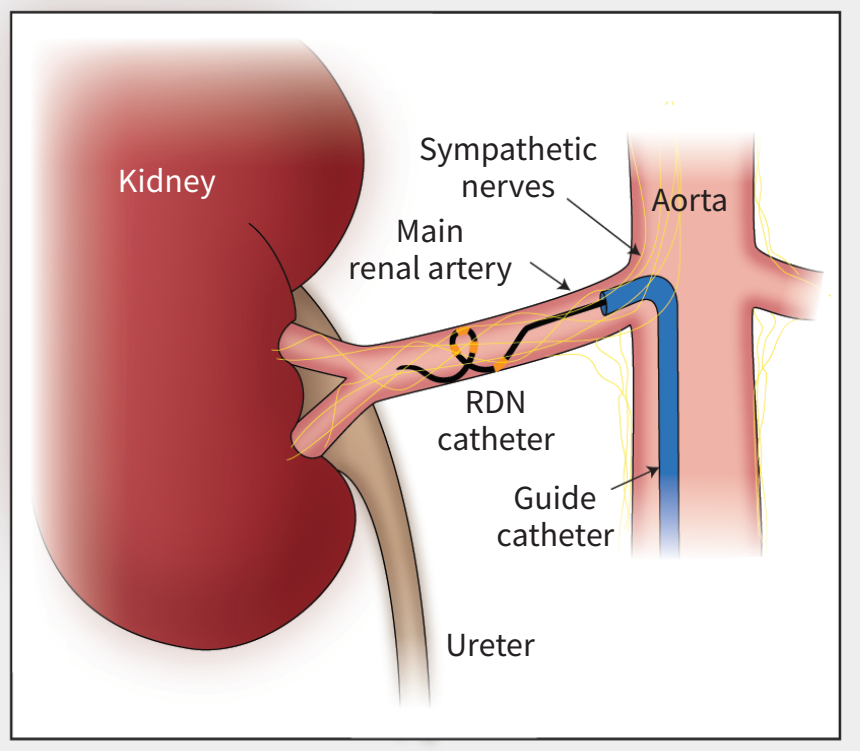
Sympathetic nervous system overdrive causes increased renal renin excretion, which results in increased blood volume and arterial tone.
-
Afferent and efferent renal nerves travel in close proximity to the renal arteries in the perivascular adipose tissue.
-
In clinical trials, renal denervation reduced systolic BP by an average of 10-12 mmHg from baseline SBP and 4–6 mm Hg over sham-controlled patients.
-
Sunnybrook uses Medtronic Symplicity G3 generator and multielectrode RDN catheter simultaneously delivers 60 seconds of radiofrequency energy to 4 gold electrodes in contact with the arterial wall in spiral configuration.

-
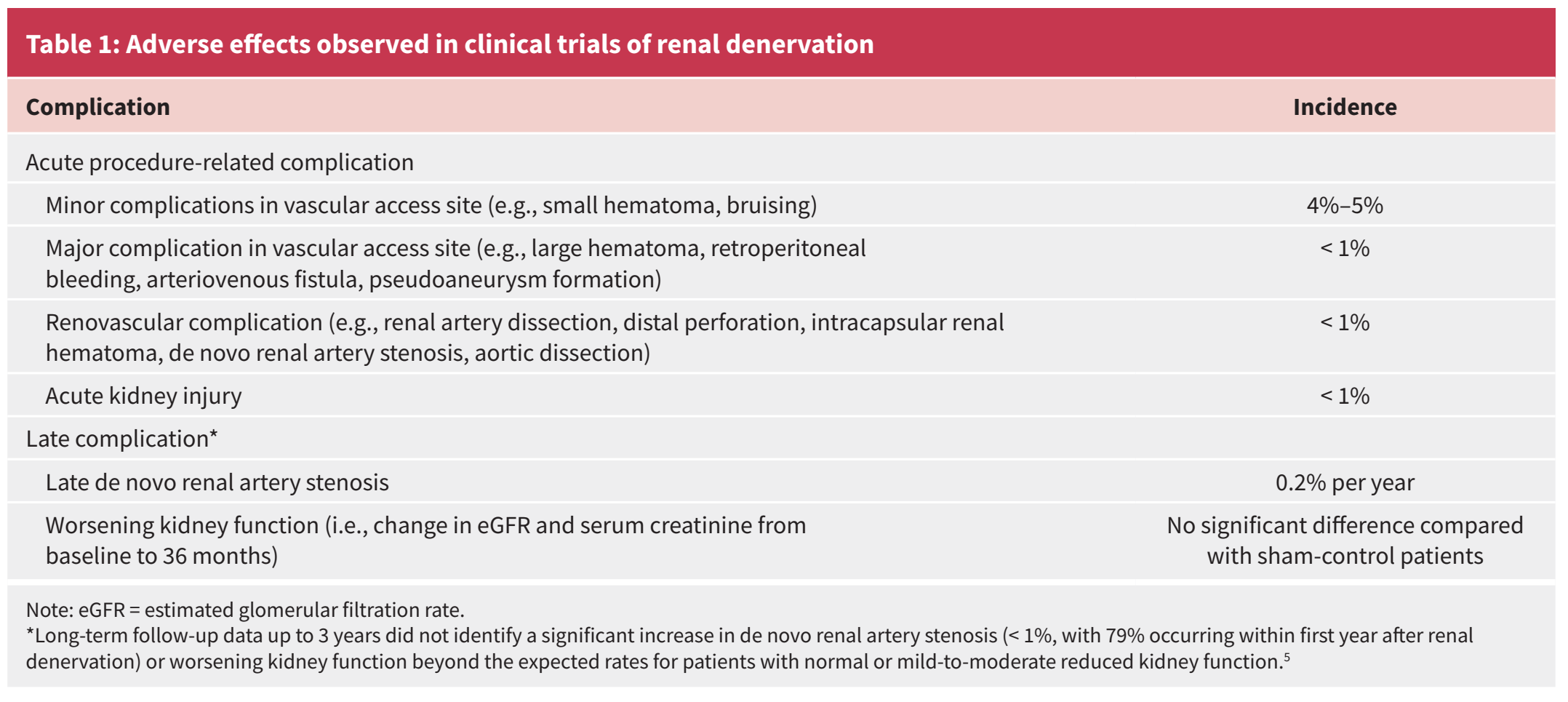
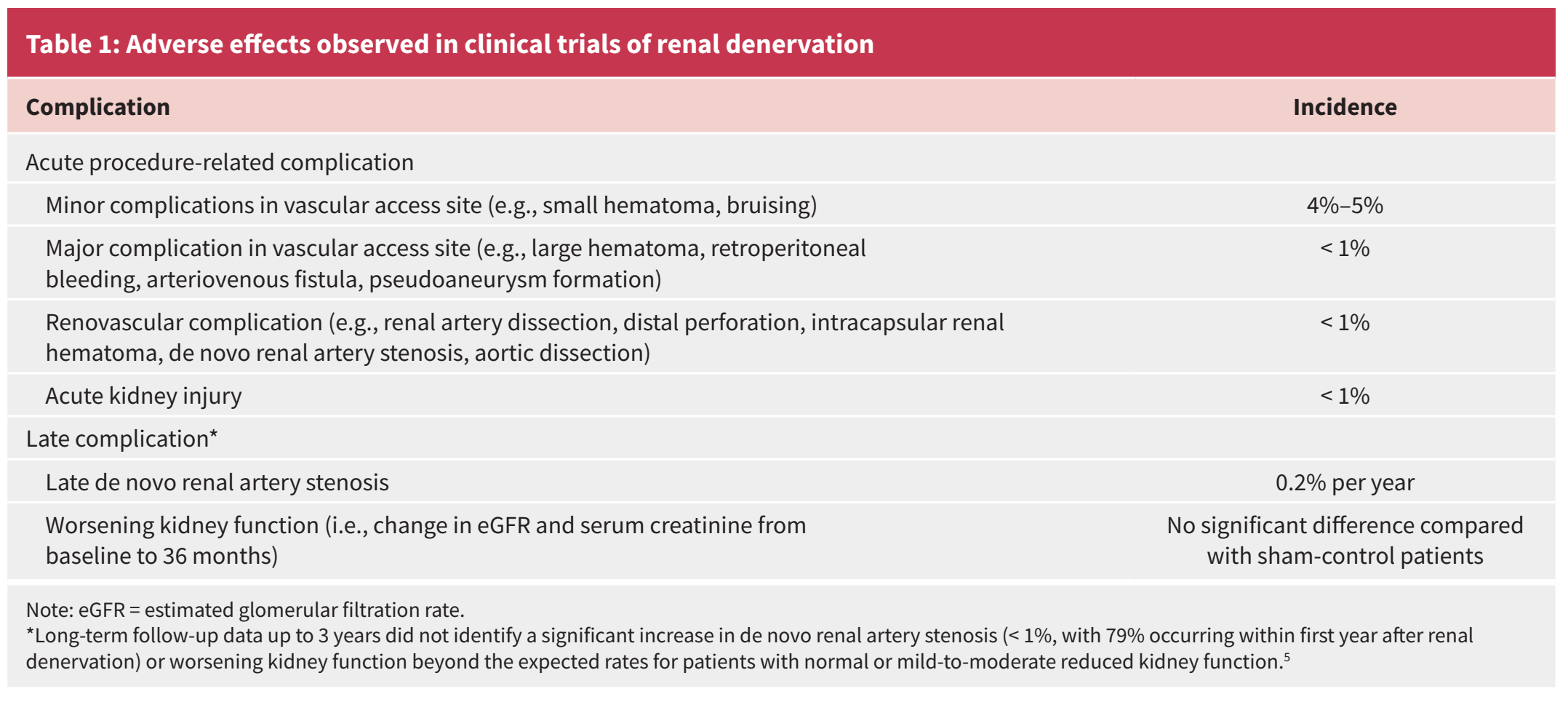
Complication is rare, mainly related to vascular access.
-
Review articles:

No Comments